2. Taylor francis 🧠: over 2500+ questions licenced from 18 text-books worth £191
3. Past examiners 🫁: Questions written by previous Medical School examiners
4. Track your performance 🏃♀️: QBank uses intelegent software to keep you on track
The reviews are in
★★★★★
6,893 users
Don't take our word for it
"The stations you provide are strikingly similar to those I came across during my medical school finals (some even verbatim!), and I have tried many other exam platforms. I'm truly grateful for your priceless support throughout my final couple of years at medical school!"
Raza Q 🇬🇧
"It has absolutely everything for medical school, so many histories with detailed differential diagnoses, how to approach emergencies, commonly prescribed drugs..every kind go examination you’ll ever need in osces"
John R 🇬🇧
"Thank you SO MUCH for the amazing educational resource. I’ve tried lots of platforms and books with mock OSCE stations and yours is by far and away the best I’ve tried"
Ed M 🇳🇿
"Get this right away. So helpful for OSCEs but also general clinical learning and understanding. Wish I had brought it sooner"
Emma W 🇬🇧
"Without a doubt, your platform outshines all other OSCE resources currently available. In all honesty, I can confidently attribute my success in securing a distinction in my finals to OSCEstop."
Harish K 🇬🇧
"OSCEstop distinguishes itself from many other platform banks by offering a wealth of questions that mimic the demanding and complex aspects of our finals. This platform played a crucial role in ensuring I was ready for the level of difficulty that awaited me in my final exams."
Membership includes access to all 4 parts of the site:
1. Learning 📖: All notes, viva questions, track progress
2. Stations 🏥: 10 years of past medical school stations. Includes: heart murmurs, ECGs, ABGs, CXR
3. Qbank 🧠: 2500+ questions from Taylor Francis books, complete MLA coverage
4. Conditions 🫀: all conditions mapped to MLA, progress tracking
The reviews are in
★★★★★
6,893 users
Don't take our word for it
"The stations you provide are strikingly similar to those I came across during my medical school finals (some even verbatim!), and I have tried many other exam platforms. I'm truly grateful for your priceless support throughout my final couple of years at medical school!"
Raza Q 🇬🇧
"It has absolutely everything for medical school, so many histories with detailed differential diagnoses, how to approach emergencies, commonly prescribed drugs..every kind go examination you’ll ever need in osces"
John R 🇬🇧
"Thank you SO MUCH for the amazing educational resource. I’ve tried lots of platforms and books with mock OSCE stations and yours is by far and away the best I’ve tried"
Ed M 🇳🇿
"Get this right away. So helpful for OSCEs but also general clinical learning and understanding. Wish I had brought it sooner"
Emma W 🇬🇧
"Without a doubt, your platform outshines all other OSCE resources currently available. In all honesty, I can confidently attribute my success in securing a distinction in my finals to OSCEstop."
Harish K 🇬🇧
"OSCEstop distinguishes itself from many other platform banks by offering a wealth of questions that mimic the demanding and complex aspects of our finals. This platform played a crucial role in ensuring I was ready for the level of difficulty that awaited me in my final exams."
Please note OSCEstop content is for educational purposes only and not intended to inform clinical practice. OSCEstop and authors take no responsibility for errors or the use of any information displayed.Drugs and doses are intended for non-pregnant adults, who are not breastfeeding, with normal renal and hepatic function.
Urea and creatinine
Physiology
Creatinine
Creatine is a substance produced primarily by the liver
Creatine is phosphorylated to creatine phosphate, which is used as an energy store for muscles
To produce energy, creatine phosphate is broken down to creatine and phosphate, which allows ADP to be converted to ATP
Creatine is metabolised to the waste product creatinine, which passes to the kidneys where it is excreted
Changes in creatinine concentration are fairly specific for determining kidney injury, but baseline level depends on muscle mass
Urea
Ammonia is a toxic waste product produced during amino acid catabolism
Ammonia is converted to urea in the liver by the ‘urea cycle’
Urea then passes to the kidneys where it is excreted
Serum urea concentration also rises in kidney injury but it is not specific for this. Other causes of high/low urea include:
↑urea = dehydration, GI bleeding, increased protein breakdown (trauma, infection, malignancy), high protein intake
↓urea = malnutrition, liver disease, pregnancy
Acute kidney injury
Acute kidney injury (AKI) = rise in serum creatinine >50% from baseline, or urine output <0.5ml/kg/hour for 6 hours.
Determine if AKI is pre-renal, renal, or post-renal.
ALL patients need:
Urine dipstick (interpreted in context of history)
Urgent renal biopsy if rapidly progressive glomerulonephritis suspected (suggested by rapid loss of kidney function, worsening severe proteinuria/haematuria, and nephritic syndrome)
Treat cause, for example:
Stop causative agent for acute interstitial nephritis
Corticosteroids, diuretics and ACE inhibitor may be required for glomerulonephritis
Post-renal AKI (10%) – caused by obstruction of the urinary tract
Plasma osmolality (to confirm if true hyponatraemia) + glucose
Low = true hyponatraemia
Normal = false hyponatraemia (‘pseudohyponatraemia’ due to hyperlipidaemia or hyperproteinemia)
High = dilutional (due to hyperglycaemia, e.g. in hyperosmolar hyperglycaemic state/DKA; alcohols; or mannitol)
Urinary sodium and osmolality (to determine whether the problem is occurring in the kidneys or elsewhere)
Specific tests to investigate for specific causes, for example:
SIADH: low plasma osmolality (<275) with high urine osmolality (>100) and high urine sodium (>30); investigate cause
Adrenal insufficiency: 9am cortisol screening test, Synacthen (synthetic ACTH) test
Hypothyroidism: TFTs
Check TFTs and 9am cortisol in all euvolaemic patients
Management
Treat cause
Sodium correction
Severe symptoms (e.g. vomiting, seizures, low GCS), regardless of cause: consider 3% hypertonic saline (e.g. 150ml over 20 minutes, repeated if necessary), usually in ICU with close monitoring
Hypovolaemic: replace lost fluid with 0.9% saline/Hartmann’s solution – slowly if chronic, e.g. 1L over 12 hours
Euvolaemic: treat cause
If SIADH or oedematous: fluid restrict to 1 litre/day (excess H2O causes dilutional hyponatraemia); consider demeclocycline (± tolvaptan) for fluid restriction-resistant SIADH; diuretics for heart failure
NB: chronic hyponatraemia (onset over 48 hours) must be corrected slowly, i.e. maximum 10mmol/L change in 24 hours (risk of osmotic change causing osmotic demyelination syndrome).
Hypernatraemia
→ thirst, confusion, muscle twitching/spasms
Causes
Euvolaemic =iatrogenic (e.g. excess IV sodium-containing fluids, sodium-containing drugs)
Hypovolaemic
Producing small volumes of concentrated urine (normal response to hypovolaemia) = dehydration
Not producing small volumes of concentrated urine (abnormal response to hypovolaemia)
Osmotic diuresis, e.g. due to hyperglycaemiaor osmotic diuretics (kidneys losing H20 and solutes)
Investigation
Urine and serum osmolality
Fluid deprivation test to confirm diabetes insipidus
Management
Treat cause
Sodium correction
Hypovolaemic (signs include hypotension, tachycardia, orthostatic hypotension): replace deficit with 0.9% saline/Hartmann’s solution
Euvolaemic: 5% dextrose – slowly if chronic, e.g. 1L over 12 hours
NB: chronic hypernatraemia (onset over 48 hours) must be corrected slowly, i.e. maximum 10mmol/L change in 24 hours (risk of osmotic change causing osmotic demyelination syndrome).
NB: may be due to pseudohyperkalaemia (haemolysis/EDTA-contaminated sample).
Management
Acute management
ECG and 3-lead cardiac monitoring
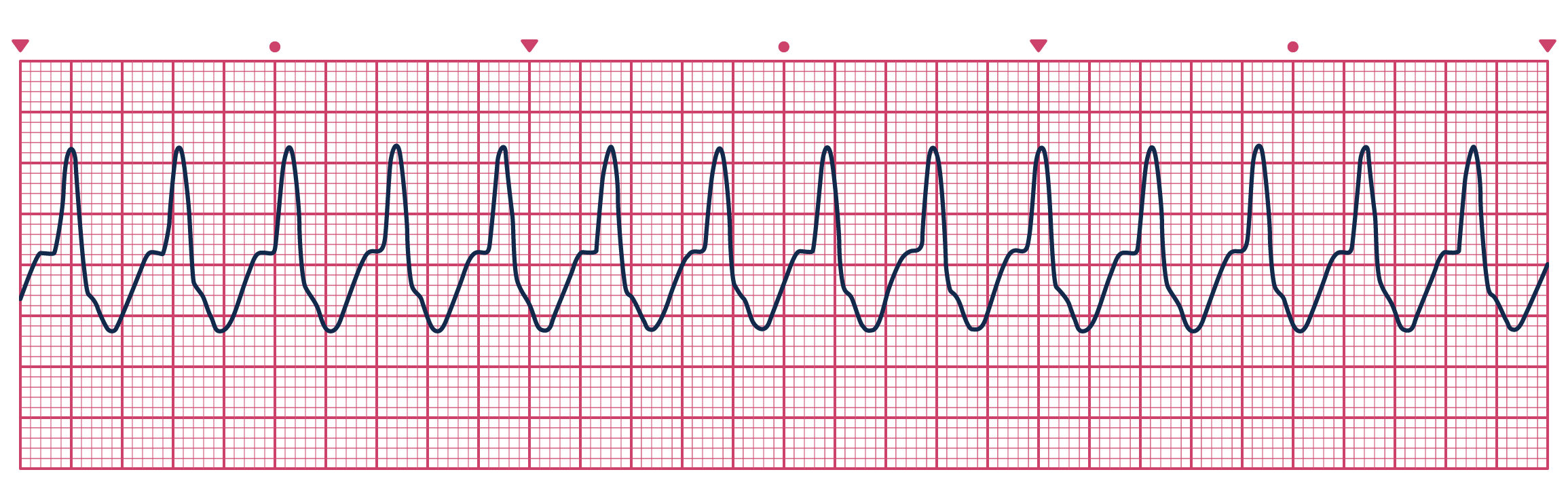
Changes: flat wide P waves, wide bizarre QRS, tall tented T waves
Calcium gluconate 30ml 10% IV over 15 minutes
Protects myocytes (required if there are ECG changes; also consider if severe, i.e. ≥6.5mmol/L, without ECG changes)
Works in minutes – check ECG changes resolved; repeat dose if no effect within 10 minutes
Lasts 30-60 minutes
Actrapid insulin 10 units in 125ml 20% dextrose IV over 30 minutes + 10mg salbutamol neb
Temporarily shifts potassium into cells
There is a risk of hypoglycaemia: monitor capillary glucose before, during and regularly after. Consider giving 10% glucose infusion at 50ml/h for 5 hours after, if the pre-treatment capillary glucose is <7mmol/L.
Gradually decreases potassium and lasts 1-2 hours, after which there is usually a slow rebound
Check K+ has normalised after 2 hours (dose can be repeated if not) and check again a few hours later
Nebulised salbutamol may be used in addition for similar but lesser effect – lasts 2 hours
Sodium zirconium cyclosilicate 10g PO TDS for up to 72 hours
Works slowly
Only treatment that actually removes potassium from body
May start with this if only moderate hyperkalaemia, i.e. K+ ≤ 5.9mmol/L
Consider renal replacement therapy if above fails (also consider sodium bicarbonate in severe acidosis)
Hypomagnesaemia (magnesium is required for PTH secretion)
Cinacalcet
Vitamin D deficiency (↓PO43-, ↑PTH)
Increased deposition in bones
Bisphosphonates
Other causes (↑PO43-, ↑PTH)
Chronic kidney disease (inability to hydroxylate 25-OH vitamin D and calcium binding to retained phosphate)
Pseudohypoparathyroidism (resistance to PTH)
Rhabdomyolysis/tumour lysis syndrome (calcium binds to high phosphate)
Investigation
Initial tests
Renal function
PTH
Phosphate, magnesium
Management
Severe (<1.9mmol/L or symptomatic): calcium gluconate 10-20ml 10% in 50-100ml 5% dextrose IV over 10 minutes with cardiac monitoring – may be repeated until asymptomatic and can be followed by an infusion if required (50ml 10% calcium gluconate in 500ml 0.9% saline or 5% dextrose at 50-100ml/hour)
Treat cause: in severe vitamin D deficiency, load with 50,000 units colecalciferol once weekly for 6 weeks; in mild vitamin D deficiency, give 800 units once daily long-term; or, if calcium and vitamin D deficient, give Adcal-D3 long-term; in end-stage CKD-associated vitamin D deficiency, use alfacalcidol (1-α hydroxycholecalciferol) instead because the kidney disease impairs the terminal hydroxylation required for vitamin D synthesis.
Drugs that decrease renal excretion (e.g. thiazide diuretics)
NB: dehydration is also a common cause. (Urea and albumin also likely raised.)
Investigation
Investigate for cause if not clear:
Initial tests: renal function, ALP, PTH, phosphate, vitamin D
Myeloma screen
CT chest, abdomen and pelvis and/or isotope bone scan (if malignancy/bony metastasis suspected)
Management
IV fluids: replace fluid deficit and keep patient well hydrated (e.g. . 0.9% saline 4-6L in 24 hours)
IV bisphosphonate (e.g. zoledronic acid 4mg IV): may be used in severe hypercalcaemia (>3.5mmol/L or symptomatic) if calcium stops falling with IV fluids alone. One-off dose; generally takes a few days to work. Dose may be reduced for poor renal function.
GI loss, e.g. severe diarrhoea, vomiting, NG losses, proton pump inhibitors
Renal loss, e.g. ketoacidosis, renal tubular diseases, hyperaldosteronism, diuretics, aminoglycosides
NB: hypomagnesaemia can cause hypokalaemia (magnesium normally inhibits renal potassium excretion) and hypocalcaemia (magnesium is required for PTH secretion and sensitivity)
Management
PO: magnesium aspartate 1 sachet (10mmol) BD x 3/7
IV:5grams (20mmol) magnesium in 500ml 0.9% saline over 5 hours
Correct hypomagnesaemia before concurrent hypokalaemia and hypocalcaemia if possible
Phosphate
Hypophosphataemia
→ lethargy, muscle weakness (skeletal, cardiac and diaphragmatic), change in mental state
Causes
Reduced intake/absorption
Vitamin D deficiency
Poor nutrition
Malabsorption (including due to alcoholism and drugs, e.g. antacids)
Increased use (phosphate shifts into cells to produce ATP from ADP for energy stores)
Refeeding syndrome
Insulin therapy
Alkalosis
Excess renal loss
Primary hyperparathyroidism
Renal tubular diseases
Management
PO: Phosphate-Sandoz 2 tablets TDS x 3/7
IV: no guidelines or licenced preparations and practice varies. Use local guidelines. Example options: Phosphate Polyfusor (50mmol in 500ml), 100-300ml over 12-24 hours depending on severity and patient weight or sodium glycerophosphate 10mmol in 500ml 0.9% saline over 12 hours – must give through different cannula to other electrolytes if co-administering
A patient presents with worsening right heart failure with extensive peripheral oedema. She normally takes bumetanide 1mg BD, eplerenone 25mg OD and ramipril 2.5mg OD. Blood tests are taken: Na+ 120, K+ 4, Ur 14, Cr 288. Her kidney function and sodium were normal when last checked 6 months ago.
What abnormalities have you identified on the blood test and what is the likely reason for them?
You are on an acute medical unit shift. You are reviewing a patient referred in by their GP. The patient is a 42 year old with a history of recurrent UTIs, for which she takes prophylactic nitrofurantoin. She had a blood test because she was feeling tired. She was referred in due to the results, which showed: Na+ 144, K+ 6.9, Ur 25, Cr 780. The patient is systemically well and observations are normal. She appears euvolaemic.



Nice notes☝️
Thanks Sylvia for your valuable comment, glad you’re enjoying the site!