2. Taylor francis 🧠: over 2500+ questions licenced from 18 text-books worth £191
3. Past examiners 🫁: Questions written by previous Medical School examiners
4. Track your performance 🏃♀️: QBank uses intelegent software to keep you on track
The reviews are in
★★★★★
6,893 users
Don't take our word for it
"The stations you provide are strikingly similar to those I came across during my medical school finals (some even verbatim!), and I have tried many other exam platforms. I'm truly grateful for your priceless support throughout my final couple of years at medical school!"
Raza Q 🇬🇧
"It has absolutely everything for medical school, so many histories with detailed differential diagnoses, how to approach emergencies, commonly prescribed drugs..every kind go examination you’ll ever need in osces"
John R 🇬🇧
"Thank you SO MUCH for the amazing educational resource. I’ve tried lots of platforms and books with mock OSCE stations and yours is by far and away the best I’ve tried"
Ed M 🇳🇿
"Get this right away. So helpful for OSCEs but also general clinical learning and understanding. Wish I had brought it sooner"
Emma W 🇬🇧
"Without a doubt, your platform outshines all other OSCE resources currently available. In all honesty, I can confidently attribute my success in securing a distinction in my finals to OSCEstop."
Harish K 🇬🇧
"OSCEstop distinguishes itself from many other platform banks by offering a wealth of questions that mimic the demanding and complex aspects of our finals. This platform played a crucial role in ensuring I was ready for the level of difficulty that awaited me in my final exams."
Membership includes access to all 4 parts of the site:
1. Learning 📖: All notes, viva questions, track progress
2. Stations 🏥: 10 years of past medical school stations. Includes: heart murmurs, ECGs, ABGs, CXR
3. Qbank 🧠: 2500+ questions from Taylor Francis books, complete MLA coverage
4. Conditions 🫀: all conditions mapped to MLA, progress tracking
The reviews are in
★★★★★
6,893 users
Don't take our word for it
"The stations you provide are strikingly similar to those I came across during my medical school finals (some even verbatim!), and I have tried many other exam platforms. I'm truly grateful for your priceless support throughout my final couple of years at medical school!"
Raza Q 🇬🇧
"It has absolutely everything for medical school, so many histories with detailed differential diagnoses, how to approach emergencies, commonly prescribed drugs..every kind go examination you’ll ever need in osces"
John R 🇬🇧
"Thank you SO MUCH for the amazing educational resource. I’ve tried lots of platforms and books with mock OSCE stations and yours is by far and away the best I’ve tried"
Ed M 🇳🇿
"Get this right away. So helpful for OSCEs but also general clinical learning and understanding. Wish I had brought it sooner"
Emma W 🇬🇧
"Without a doubt, your platform outshines all other OSCE resources currently available. In all honesty, I can confidently attribute my success in securing a distinction in my finals to OSCEstop."
Harish K 🇬🇧
"OSCEstop distinguishes itself from many other platform banks by offering a wealth of questions that mimic the demanding and complex aspects of our finals. This platform played a crucial role in ensuring I was ready for the level of difficulty that awaited me in my final exams."
Haemoglobin (Hb): concentration of haemoglobin within the blood. Hb is the protein in red blood cells which carries oxygen. It is the first value you should look at. Low haemoglobin = ‘anaemia’.
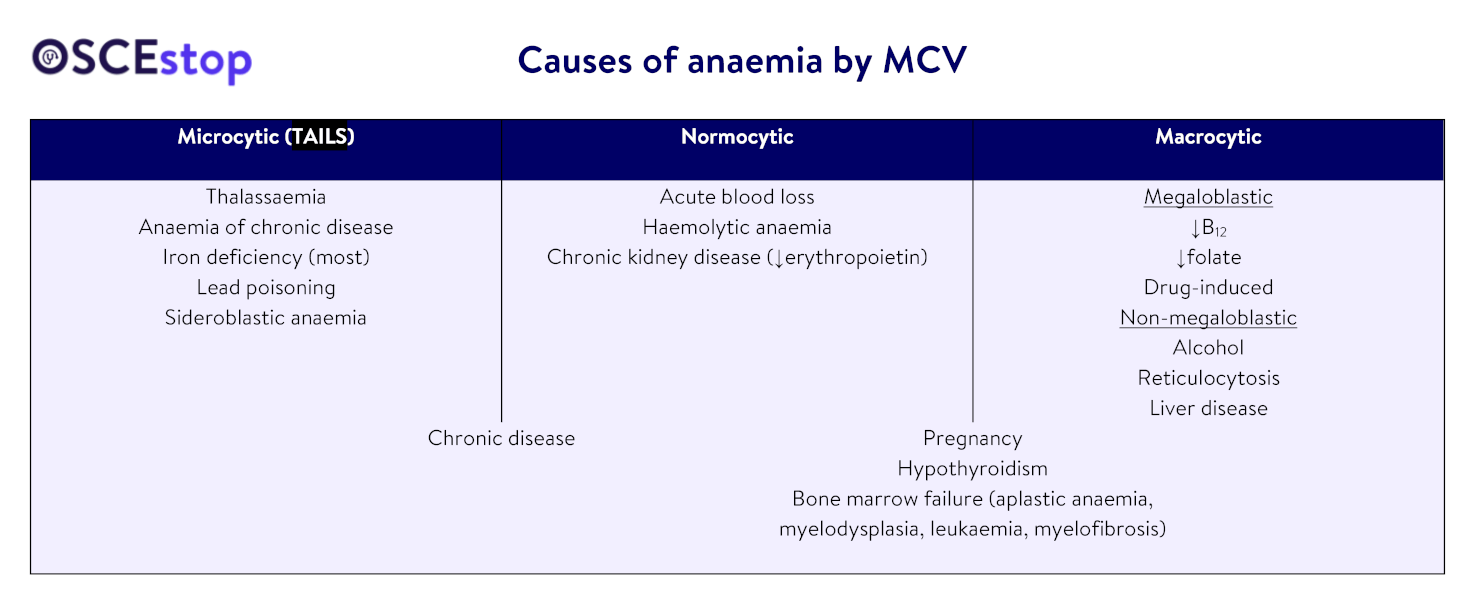
Mean corpuscular volume (MCV): mean volume of the red blood cells (‘-cytic’). This is the main method used to classify anaemia (macrocytic = large cells; normocytic = normal cells; microcytic = small cells).
Reticulocyte count: the number of immature red blood cells. Increased in blood loss and haemolytic anaemia because the bone marrow works harder to replace lost cells. Decreased if there is impaired red blood cell production in the bone marrow.
Red cell count (RCC): the concentration of red blood cells within the blood
It may be increased due to: reduced plasma volume (e.g. dehydration), or increased red blood cell production (e.g. polycythaemia rubra vera)
It may be decreased due to: increased plasma volume (e.g. pregnancy), or reduced red blood cell production/red blood cell loss (e.g. bone marrow failure, bleeding, anaemias)
Haematocrit (HCT)/packed cell volume (PCV):percentage of the total volume of blood accounted for by red blood cells. Causes of abnormalities are similar to the RCC but the haematocrit is based on volume so is also affected by the red cell volume (MCV).
Mean corpuscular haemoglobin (MCH)/haemoglobin concentration (MCHC): the mean quantity/concentration of haemoglobin within the red bloods cells. This affects the colour of the cells (‘-chromic’: hypochromic = pale; normochromic = normal red).
Most normocytic and macrocytic anaemias are normochromic
Most microcytic anaemias are hypochromic (except anaemia of chronic disease)
Red blood cell distribution width (RDW): measure of the variation of red blood cell volumes. It is used in conjunction with MCV to determine if anaemia is due to a mixed cause or a single cause. Raised red cell distribution width = ‘anisocytosis’.
Anaemia
Anaemia = a reduced concentration of haemoglobin within the blood.
Other relevant tests:
WCC and platelet count: if both are also abnormal, a bone marrow cause is likely
Reticulocyte count: if raised, the cause isblood loss or haemolytic anaemia
Mean corpuscular volume (MCV):
Tests for specific causes
Haematinics: B12, folate and ferritin(NB: ferritin is also an acute phase proteinso may be falsely elevated due inflammation)
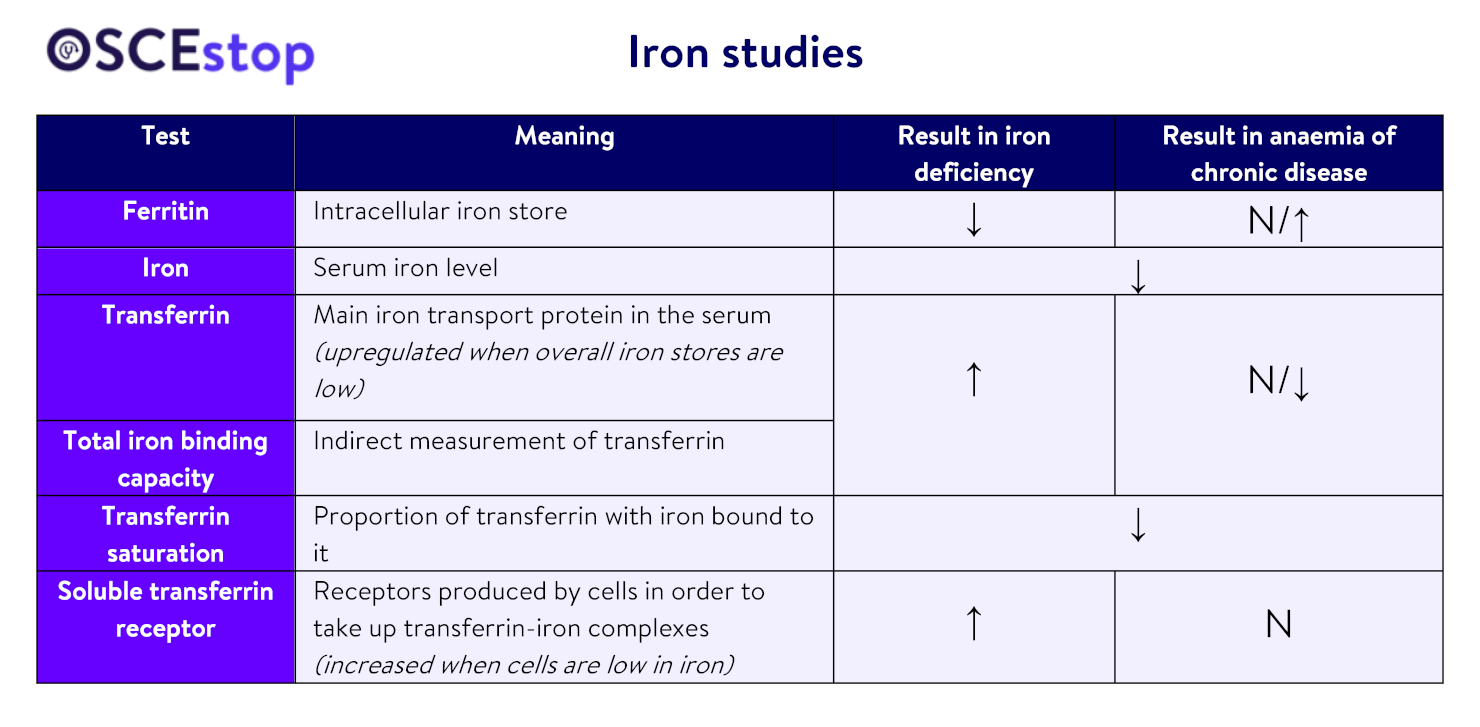
Iron studies: see table below
TFTs
Bilirubin (unconjugated bilirubin is raised in haemolysis)
Bloodfilm ± bone marrow biopsy (if bone marrow cause/sideroblastic anaemia suspected)
NB. A low ferritin is consistent with iron-deficiency but a normal ferritin cannot exclude iron-deficiency if there is acute/chronic inflammation because ferritin is an acute phase reactant.
Commonest causes
Iron-deficiency anaemia
Physiology: iron is found in meats and fish as haem iron, and in cereals, green vegetables and beans as non-haem iron. In humans, 2/3 is stored as haem, 2/9 as ferritin and 1/9 as haemosiderin.
Causes:
Chronic blood loss (from GI tract, e.g. malignancy/inflammation/ulcers/varices/haemorrhoids; or menorrhagia)
Investigations if no clear cause: OGD + colonoscopy, coeliac screen, urine dip
Treatment: treat cause, iron supplementation (infusion/ferrous sulphate/fumarate tablets), transfusion if Hb<70
B12-deficiency anaemia
Physiology: vitamin B12 is found in meat and dairy products. The stomach produces intrinsic factor which binds to B12, allowing it to be absorbed in the terminal ileum. Body stores last up to 4 years.
Investigations for pernicious anaemia: parietal cell antibodies, intrinsic factor antibodies, Schilling’s test (rarely used)
Treatment: treat cause; hydroxocobalamin (B12) injections 3-monthly, or oral vitamin B12 may be used if dietary deficiency
Folate-deficiency anaemia
Physiology: folate is found in green vegetables and fortified cereals. Body stores only last 4 months and deficiency develops earlier in malabsorption/pregnancy.
Causes:
Dietary (alcoholism, neglect, poor diet)
↑ requirements (pregnancy, haematopoiesis)
Malabsorption in small bowel (coeliac disease, pancreatic insufficiency, Crohn’s disease, tropical sprue)
Drugs that interfere with metabolism (phenytoin, methotrexate, trimethoprim)
NB: in coexistent B12 and folate deficiency, always treat B12 first to prevent subacute combined degeneration of the cord. (Treat in alphabetical order!)
Anaemia of chronic disease
See iron studies table above
Physiology: inflammatory cytokines reduce the ability of bone marrow to respond to erythropoietin, leading to anaemia. They also reduce cellular iron release, which reduces the serum iron level and also results in lower transferrin saturation. Ferritin (intracellular iron store) is still normal/high, and transferrin and cellular soluble transferrin receptors are not upregulated because overall body iron stores are normal.
Causes: any chronic disease
Treatment: treat cause, transfuse if Hb<70
Haemolytic anaemia
Physiology:
Normally, red cells are destroyed extravascularly by macrophages with the following effects:
Hb → globulin (which is broken down into amino acids) + haem (which is broken down into bilirubin)
Bilirubin is then conjugated by the liver (a rate-limited process), and released as bile into the bowel, where it is converted to urobilinogen
Some urobilinogen is passed in stool; the rest is reabsorbed and excreted in urine as urinary urobilinogen
However, if red cells are destroyed intravascularly (pathological), free Hb follows one of three pathways:
Some binds to haptoglobin (and is removed by liver)
Some is filtered by the glomerulus and passed as haemoglobinuria or haemosiderinuria
Some is oxidised to methaemoglobin which dissociates into globin + ferriheme (most ferriheme then binds to albumin → methaemalbuminaemia)
Enzyme assays, e.g. G6PD, pyruvate kinase (for enzyme defects)
Polycythaemia
Polycythaemia = increased volume percentage of red blood cells within the blood.
Causes
Relative polycythaemia (i.e. ↓ plasma volume)
Acute dehydration
Chronic (associated with obesity, hypertension, alcohol excess, smoking)
Absolute polycythaemia (i.e. ↑ red blood cells)
Primary = polycythaemia rubra vera
Secondary = due to increased erythropoietin because of chronic hypoxaemia (e.g. COPD, altitude, congenital cyanotic heart disease) or erythropoietin-secreting tumours (e.g. renal cell carcinoma)
Investigations
WCC and platelet count (both also raised in primary absolute polycythaemia, but not in secondary absolute polycythaemia)
Erythropoietin level
If polycythaemia rubra vera suspected: request JAK-2 mutation testing and consider bone marrow biopsy