2. Taylor francis 🧠: over 2500+ questions licenced from 18 text-books worth £191
3. Past examiners 🫁: Questions written by previous Medical School examiners
4. Track your performance 🏃♀️: QBank uses intelegent software to keep you on track
The reviews are in
★★★★★
6,893 users
Don't take our word for it
"The stations you provide are strikingly similar to those I came across during my medical school finals (some even verbatim!), and I have tried many other exam platforms. I'm truly grateful for your priceless support throughout my final couple of years at medical school!"
Raza Q 🇬🇧
"It has absolutely everything for medical school, so many histories with detailed differential diagnoses, how to approach emergencies, commonly prescribed drugs..every kind go examination you’ll ever need in osces"
John R 🇬🇧
"Thank you SO MUCH for the amazing educational resource. I’ve tried lots of platforms and books with mock OSCE stations and yours is by far and away the best I’ve tried"
Ed M 🇳🇿
"Get this right away. So helpful for OSCEs but also general clinical learning and understanding. Wish I had brought it sooner"
Emma W 🇬🇧
"Without a doubt, your platform outshines all other OSCE resources currently available. In all honesty, I can confidently attribute my success in securing a distinction in my finals to OSCEstop."
Harish K 🇬🇧
"OSCEstop distinguishes itself from many other platform banks by offering a wealth of questions that mimic the demanding and complex aspects of our finals. This platform played a crucial role in ensuring I was ready for the level of difficulty that awaited me in my final exams."
Membership includes access to all 4 parts of the site:
1. Learning 📖: All notes, viva questions, track progress
2. Stations 🏥: 10 years of past medical school stations. Includes: heart murmurs, ECGs, ABGs, CXR
3. Qbank 🧠: 2500+ questions from Taylor Francis books, complete MLA coverage
4. Conditions 🫀: all conditions mapped to MLA, progress tracking
The reviews are in
★★★★★
6,893 users
Don't take our word for it
"The stations you provide are strikingly similar to those I came across during my medical school finals (some even verbatim!), and I have tried many other exam platforms. I'm truly grateful for your priceless support throughout my final couple of years at medical school!"
Raza Q 🇬🇧
"It has absolutely everything for medical school, so many histories with detailed differential diagnoses, how to approach emergencies, commonly prescribed drugs..every kind go examination you’ll ever need in osces"
John R 🇬🇧
"Thank you SO MUCH for the amazing educational resource. I’ve tried lots of platforms and books with mock OSCE stations and yours is by far and away the best I’ve tried"
Ed M 🇳🇿
"Get this right away. So helpful for OSCEs but also general clinical learning and understanding. Wish I had brought it sooner"
Emma W 🇬🇧
"Without a doubt, your platform outshines all other OSCE resources currently available. In all honesty, I can confidently attribute my success in securing a distinction in my finals to OSCEstop."
Harish K 🇬🇧
"OSCEstop distinguishes itself from many other platform banks by offering a wealth of questions that mimic the demanding and complex aspects of our finals. This platform played a crucial role in ensuring I was ready for the level of difficulty that awaited me in my final exams."
Natural anticoagulants: proteins C and S (inactivate factors V and VIII); antithrombin (inactivates many clotting factors)
Vitamin K dependent clotting factors: II, VII, IX, X (+ proteins C and S)
Most coagulation factors are synthesised by the liver
NB: when an ‘a’ is placed after the clotting factor number (e.g. ‘factor Xa’), it means it is in its activated form.
Coagulation tests
Basic tests
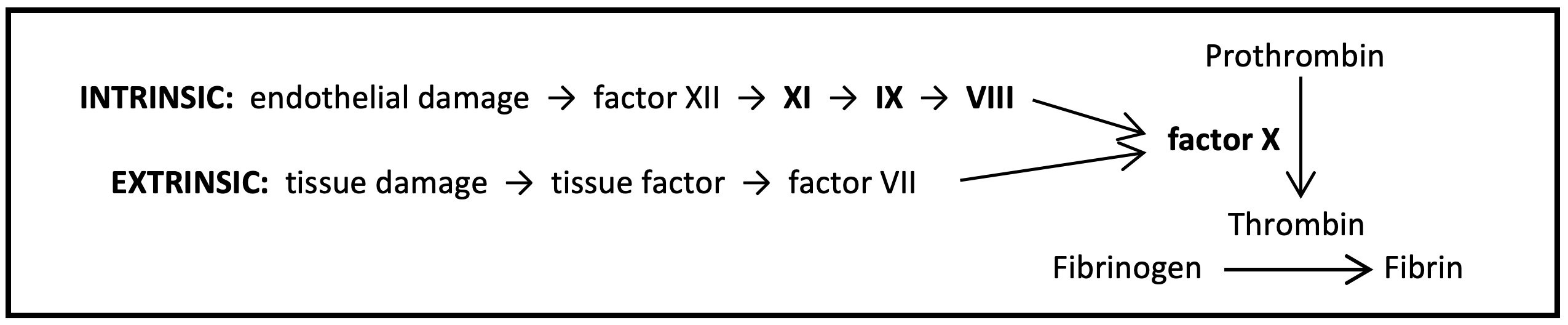
PT and INR = EXTRINSIC
Tissue factor is added to blood in the laboratory to activate the extrinsic pathway. Clotting time (PT) is measured in seconds (normal usually = 12-13). However, the PT may vary depending on the reagent used, so the laboratory can use the PT to calculate the INR to standardise results (normal = 0.8-1.2).
WEPT – Warfarin Extrinsic Prothrombin Time
Only factor VII is involved in the extrinsic pathway, before the common pathway. Isolated factor VII deficiencies are rare, so PT/INR is only really affected by globally reduced clotting factor synthesis or increased
Warfarin/vitamin K deficiency
Liver disease
Disseminated intravascular coagulation
APTT = INTRINSIC
A contact activator is added to blood in the laboratory to activate the intrinsic pathway. Clotting time (APTT) is measured in seconds (normal usually = 30-50). The APTT can be divided by the mean normal value to calculate the APTT ratio if required.
The APTT involves similar clotting factors to the extrinsic pathway PLUS others (VIII, IX, XI) so is affected by:
Warfarin/vitamin K deficiency
Liver disease
Disseminated intravascular coagulation
PLUS anything which affects factor VIII (haemophilia A/von Willebrand disease), factor IX (haemophilia B), or factor XI (haemophilia C)
NB: factor XII is also involved in the intrinsic pathway but isolated deficiencies are rare.
NB: antiphospholipid syndrome is a common cause of a misleadingly prolonged APTT, due to antibody-mediated inactivation of the phospholipid added in the laboratory to activate the intrinsic pathway.
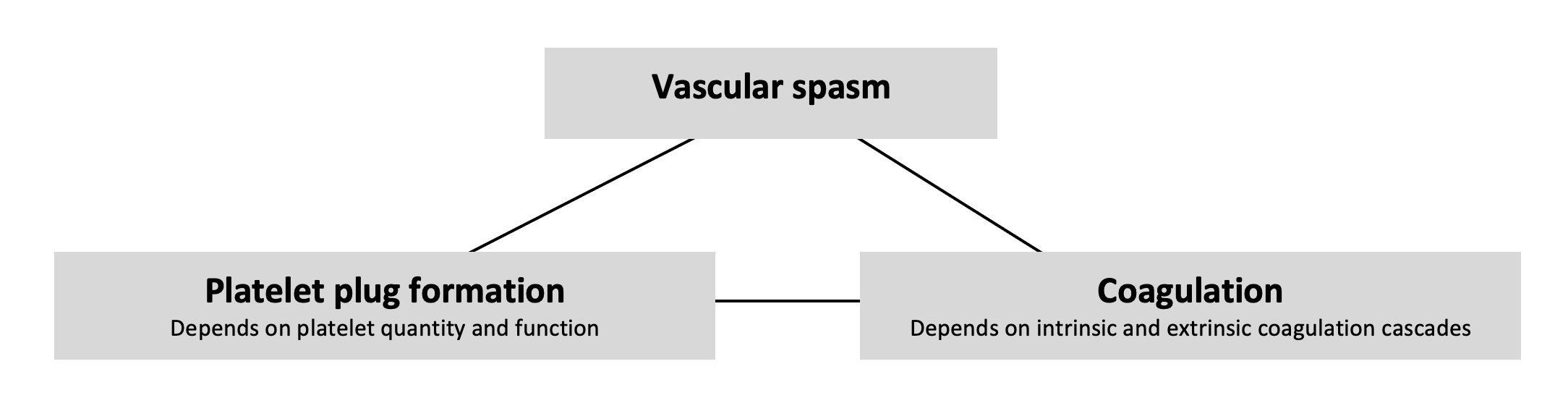
Bleeding time = PLATELET FUNCTION
Involves making an incision in the patient’s skin and timing how long it takes to stop bleeding
Measures platelet plug formation so only affected by conditions involving platelet quantity/function
Rarely used in practice
Fibrinogen
Fibrinogen is a clotting factor involved in the final stage of coagulation
The fibrinogen level reflects the blood’s clotting ability (low = increased bleeding risk; high = may increase clotting)
Low levels are due to: increased consumption (e.g. disseminated intravascular coagulation) or decreased production (e.g. liver disease, malnutrition)
Fibrinogen is an acute phase protein and high levels may be due to: inflammation, malignancy, trauma, or infection
Other relevant tests
Full blood count: to check platelet count and other haematological abnormalities
Liver function tests: to exclude liver function abnormalities as a cause for clotting problems
Antiphospholipid antibodies (e.g. lupus anticoagulant, anticardiolipin antibodies, anti-β2 glycoprotein I antibodies) – to look for antiphospholipid syndrome
Factor assays ± factor inhibitor antibodies (e.g. factors VIII, IX, XI) – the level of individual clotting factors may be tested to look for common deficiencies (e.g. haemophilia A, B, C respectively)
Important conditions
Factor synthesis problems
Vitamin K deficiency
Vitamin K is a fat-soluble vitamin so may be deficient if there is fat malabsorption (e.g. in biliary obstruction – check LFTs) or a simple dietary deficiency
Deficiency leads to reduced synthesis of vitamin K dependent clotting factors (2, 7, 9, 10) and so affects both intrinsic and extrinsic pathways
If due to dietary deficiency, treat with oral vitamin K (phytomenadione) 5-10mg OD for 3 days; if due to fat malabsorption, give IV vitamin K or oral menadiol (a water-soluble vitamin K derivative)
Liver disease
The liver synthesises most clotting factors so liver disease can result in a global deficiency, affecting both intrinsic and extrinsic pathways
Platelets may also be reduced due to hypersplenism
Liver-related coagulopathy is difficult to manage and is mainly supportive (e.g. FFP, cryoprecipitate, platelet transfusions as required). Vitamin K may be given if deficiency is suspected.
Consumption
Disseminated intravascular coagulation
In severe systemic illness, dying cells release procoagulants, resulting in fibrin generation, which can occlude small vessels
This process consumes platelets and clotting factors, resulting in bleeding elsewhere
Blood tests reveal thrombocytopenia; increased PT/INR and APTT; low fibrinogen; and raised D-dimer and fibrin degradation products
Treat the cause and give supportive therapies (e.g. blood, platelets, FFP, cryoprecipitate)
Drugs
Warfarin (vitamin K antagonist)
Reduces synthesis of vitamin K dependent clotting factors (II, VII, IX, X) and so affects both intrinsic and extrinsic pathways
Its effect is monitored using INR, which is a measure of the extrinsic pathway
It can be reversed using prothrombin complex concentrate and vitamin K
Heparin
Heparin is an anticoagulant that increases antithrombin activity by enhancing its binding to factor Xa and thrombin. Types of heparin that are commonly used include:
Subcutaneous LMWH (e.g. enoxaparin): most commonly used for prophylactic and therapeutic anticoagulation. LMWH consists of only short chain heparins, so most of its activity is mediated by inhibition of factor Xa. Its effects are therefore more predictable than those of standard (unfractionated) heparin. Monitoring is not routinely required, but its effect can be measured by anti-factor Xa assay.
IV or subcutaneous unfractionated (standard) heparin: consists of heparin chains with a variety of molecular lengths. Its effect on the coagulation cascade is therefore more wide-ranging and less predictable
Subcutaneous therapy may be used for prophylactic anticoagulation in patients with reduced renal function, since unfractionated heparin is predominately cleared by the liver, whereas LMWH is not.
IV heparin has a short half life and stops working after 4 hours. It can therefore be used for therapeutic anticoagulation peri-operatively, or if there is significant risk of bleeding. It must be monitored regularly, using the APTT ratio, and dose-adjusted according to hospital guidelines.
Both types of heparin can be reversed with protamine sulphate if required.
Deficiencies
Haemophilia
HaemophiliaA = factor VIII deficiency
HaemophiliaB = factor IX deficiency
HaemophiliaC = factor XI deficiency
Clinical features depend on levels of affected factor but characteristically include haemarthroses and muscle haematomas.
Autoimmune
Antiphospholipid syndrome
Antiphospholipid antibodies react against proteins that bind to plasma membrane phospholipids, resulting in arterial and venous thrombosis
Antiphospholipid syndrome misleadingly causes a prolonged APTT because the antibodies inactivate the phospholipid added to activate the intrinsic pathway during the laboratory measurement of APTT
A 34 year old male who was previously fit and well is referred by his GP to the Same Day Emergency Care unit with bilateral leg swelling and breathlessness. Blood tests are undertaken and are unremarkable other than a coagulation screen that reveals a significantly raised APTT (with a normal INR and fibrinogen). This is repeated and the results are the same. A CTPA confirms bilateral PEs and Dopplers of the lower limbs confirm bilateral extensive DVTs.
Based on the blood test, which clotting pathway is affected?