2. Taylor francis 🧠: over 2500+ questions licenced from 18 text-books worth £191
3. Past examiners 🫁: Questions written by previous Medical School examiners
4. Track your performance 🏃♀️: QBank uses intelegent software to keep you on track
The reviews are in
★★★★★
6,893 users
Don't take our word for it
"The stations you provide are strikingly similar to those I came across during my medical school finals (some even verbatim!), and I have tried many other exam platforms. I'm truly grateful for your priceless support throughout my final couple of years at medical school!"
Raza Q 🇬🇧
"It has absolutely everything for medical school, so many histories with detailed differential diagnoses, how to approach emergencies, commonly prescribed drugs..every kind go examination you’ll ever need in osces"
John R 🇬🇧
"Thank you SO MUCH for the amazing educational resource. I’ve tried lots of platforms and books with mock OSCE stations and yours is by far and away the best I’ve tried"
Ed M 🇳🇿
"Get this right away. So helpful for OSCEs but also general clinical learning and understanding. Wish I had brought it sooner"
Emma W 🇬🇧
"Without a doubt, your platform outshines all other OSCE resources currently available. In all honesty, I can confidently attribute my success in securing a distinction in my finals to OSCEstop."
Harish K 🇬🇧
"OSCEstop distinguishes itself from many other platform banks by offering a wealth of questions that mimic the demanding and complex aspects of our finals. This platform played a crucial role in ensuring I was ready for the level of difficulty that awaited me in my final exams."
Membership includes access to all 4 parts of the site:
1. Learning 📖: All notes, viva questions, track progress
2. Stations 🏥: 10 years of past medical school stations. Includes: heart murmurs, ECGs, ABGs, CXR
3. Qbank 🧠: 2500+ questions from Taylor Francis books, complete MLA coverage
4. Conditions 🫀: all conditions mapped to MLA, progress tracking
The reviews are in
★★★★★
6,893 users
Don't take our word for it
"The stations you provide are strikingly similar to those I came across during my medical school finals (some even verbatim!), and I have tried many other exam platforms. I'm truly grateful for your priceless support throughout my final couple of years at medical school!"
Raza Q 🇬🇧
"It has absolutely everything for medical school, so many histories with detailed differential diagnoses, how to approach emergencies, commonly prescribed drugs..every kind go examination you’ll ever need in osces"
John R 🇬🇧
"Thank you SO MUCH for the amazing educational resource. I’ve tried lots of platforms and books with mock OSCE stations and yours is by far and away the best I’ve tried"
Ed M 🇳🇿
"Get this right away. So helpful for OSCEs but also general clinical learning and understanding. Wish I had brought it sooner"
Emma W 🇬🇧
"Without a doubt, your platform outshines all other OSCE resources currently available. In all honesty, I can confidently attribute my success in securing a distinction in my finals to OSCEstop."
Harish K 🇬🇧
"OSCEstop distinguishes itself from many other platform banks by offering a wealth of questions that mimic the demanding and complex aspects of our finals. This platform played a crucial role in ensuring I was ready for the level of difficulty that awaited me in my final exams."
Please note OSCEstop content is for educational purposes only and not intended to inform clinical practice. OSCEstop and authors take no responsibility for errors or the use of any information displayed.
Normal maintenance requirements
The normal maintenance requirements for a nil by mouth patient depends on the patient’s weight (example for an average 70kg patient over 24 hours in brackets):
H2O: 1.5ml/kg/hour (2.5L)
Na+: 1-2mmol/kg/day (70-140mmol)
K+: 0.5-1mmol/kg/day (35-70mmol)
NB: urine output should be >0.5ml/kg/hour (>35ml/hour)
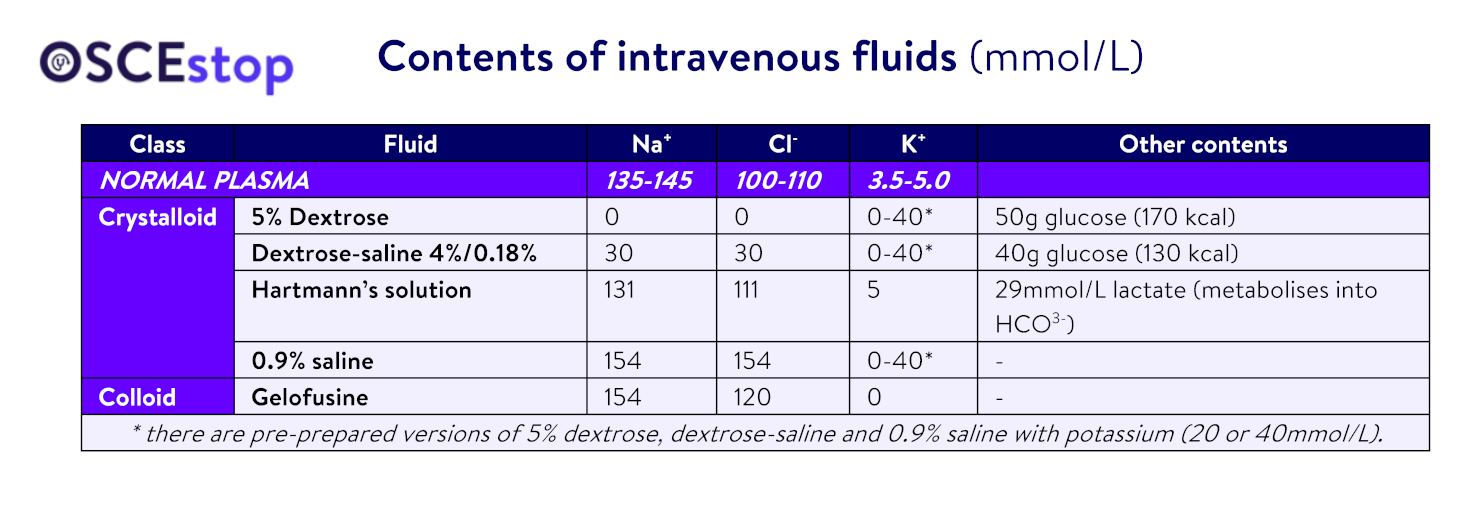
Available intravenous fluids
5% dextrose
This is given instead of pure water. The glucose is present to maintain initial osmolality but is quickly used up and plays no role thereafter (the calorific content is negligible). It is used as part of a maintenance fluid regimen, when water is required without electrolytes. It is of no use in treating hypovolaemia because it is not physiological (i.e. similar to plasma) and distributes widely across all fluid compartments. Administering too much, too quickly can cause hyponatraemia.
Dextrose-saline
This is a good choice for maintenance fluids because, when given alone at the correct maintenance rate (i.e. at 1.5ml/kg/hour), it will provide approximately the correct sodium requirement over 24 hours. Because the sodium content is much lower than that of plasma, however, it is of no use in treating hypovolaemia. Administering too much, too quickly can cause hyponatraemia.
Hartmann’s solution
This is the most physiological fluid and so is very good for replacing plasma loss, e.g. GI losses or during surgery. However, this does not mean it is good for normal maintenance fluids alone, as 3L Hartmann’s solution over 24 hours would give three times too much sodium and not enough potassium.
NB: Hartmann’s solution is also known as Ringer’s lactate solution, and similar solutions are available, such as Plasmalyte.
0.9% saline
This is much more physiological than dextrose as it contains sodium chloride, but is not as physiological as Hartmann’s solution because it contains a greater concentration than plasma. Also, be warned: too much chloride can cause a hyperchloraemic metabolic acidosis; and it can also cause renal afferent arteriole vasoconstriction (increases risk of acute kidney injury).
Notes on fluids and fluid compartments
Fluids are given intravenously and so enter the intravascular space. However, depending on the osmolality, the fluid will be distributed across the various fluid compartments (intravascular, interstitial, intracellular) to different extents.
The aim of fluid resuscitation in hypovolaemic patients is to expand the intravascular volume by administering fluids that stay in the intravascular space, such as Hartmann’s solution, 0.9% saline and colloids
The different components of the above formula should be considered separately because each may need a different fluid prescribed. When prescribing fluids, you need to be clear about what type of fluid you are prescribing, how much of it, and why. The type and quantity of maintenance fluid is based on the patient’s fluid and electrolyte requirements (dependent on their weight), and the type and quantity of replacement fluid is based on the type and quantity of fluid lost. You will usually be giving fluids for either maintenance or replacement rather than both – but you need to be clear in your own head what you are doing!
The type of fluid does not matter provided that, over 24 hours, it approximately matches the patient’s weight requirements of water, sodium and potassium. Calculate how much of all of these are needed and choose fluids which match these requirements closest. By convention, bags are given over multiples of 2 hours.
Note, there are problems with the traditional fluid regimen of ‘1 salty + 2 sweet’:
This gives 3L H20, 154mmol Na+ and 60mmol K+. This is only acceptable for a very large patient because it provides about 0.5L more water and more sodium than is required for an average patient. The fluids you give should always reflect the patient’s weight. Thus for a 70kg patient, maintenance regimens need to provide approximately 2.5L fluid, 70-140mmol Na+, and 35-70mmol K+).
Fluid losses should be replaced with fluids which have a similar electrolyte content to the fluid that has been lost. The main types of fluid loss and what they should be replaced with are:
Extracellular fluid/volume depletion, e.g. due to diarrhoea and vomiting, NG aspirates, stomas, burns, pancreatitis, sepsis: this should be replaced with a fluid similar to extracellular fluid, which is similar to plasma (e.g. Hartmann’s solution or 0.9% saline).
NB: if a patient needs a lot of sodium-rich fluid resuscitation, Hartmann’s solution is preferred to 0.9% saline because it contains less chloride (too much chloride causes a hyperchloraemic acidosis).
Dehydration/total water loss, e.g. due to poor intake: should be replaced by normal maintenance-type fluids (e.g. dextrose-saline). However, if these patients are hypotensive and need a fluid bolus, use Hartmann’s solution or 0.9% saline, because a larger volume will stay in the intravascular space.
Blood loss: should be replaced with blood. If the patient continues to bleed, they may also need other products, e.g. FFP/platelets to stop the bleeding rather than just replace the lost red cells.
Two components need to be considered when replacing fluid losses:
Pre-existing fluid deficit (replaced using STAT boluses)
Ongoing losses (prescribe fluids to replace future losses as they are likely to occur)
Pre-existing fluid deficit
The quantity of fluid replacement depends on your estimate of the fluid deficit. Determine the approximate deficit and the cause by:
The history
Observations, fluid balance chart and hydration status examination
U&Es: but be aware this is a measurement of plasma levels and may not represent total body stores (because homeostasis mechanisms keep plasma levels within a certain range)
Classes of shock:
Shock class
Fluid lost
Signs
1
0.75L (15%)
Minimal, mild tachycardia
2
0.75-1.5L (15-30%)
Moderate tachycardia, prolonged capillary refill
3
1.5-2L (30-40%)
Severe tachycardia and hypotension, confusion
4
>2L (>40%)
Critical tachycardia and hypotension
Fluid resuscitation to replace pre-existing deficits is delivered in STAT boluses. 500ml 0.9% saline/Hartmann’s solution is a good choice. You must reassess the patient’s fluid status (including blood pressure and urine output) after each bolus to guide further fluid resuscitation. If they require large fluid volumes, also regularly assess for signs of fluid overload (e.g. raised JVP, increasing oxygen requirements, peripheral/pulmonary oedema).
For acutely hypotensive patients when you are unsure of the exact cause or quantity of fluid loss, unless you suspect heart failure, give a fluid challenge and then assess the response:
↘respond fully: just prescribe fluids for future losses/maintenance
↘respond and become hypotensive again: give more resuscitation fluids (amount depends on patient but usually around 20ml/kg quickly)
↘no response: patient may be very depleted (give lots of fluids), or in heart failure (don’t give any more fluids) – assess clinically and look for signs of fluid overload such as raised JVP and pulmonary/peripheral oedema
WARNING: be cautious if the patient has a history of heart failure history and use only 250ml fluid challenges. Bear in mind heart failure patients may normally run hypotensive. If there are signs of heart failure, DO NOT give fluids – ask for senior advice because diuretics or inotropes may be required.
Ongoing losses
You must estimate these and aim to prescribe a regimen to replace them as they occur with a type of fluid similar in electrolyte content to what is being lost.
Special situations
Post-operatively
K+ stores are mostly intracellular and serum levels can increase due to cell lysis during surgery. Hence, if K+ is over 4.5mmol/L post-operatively, omit it from the fluid prescription for 24 hours.
If K+ is normal/low, you can give some, e.g. 40mmol in 24 hours. 0.9% saline is generally avoided where possible post-operatively because surgery and trauma trigger the renin-angiotensin-aldosterone system (which causes sodium and fluid retention and reduced urine output), and because sodium-containing substances are often given in theatre (e.g. colloids, Hartmann’s solution and IV antibiotics).
Too much sodium chloride can result in oedema, hyperchloraemic acidosis, increased kidney load, increased post-operative complications, and GI problems. Dextrose-saline contains less sodium chloride and so is preferred for maintenance fluid instead.
Sepsis
Sepsis causes intravascular depletion due to plasma loss through leaky capillaries and vasodilation. Replace fluid with Hartmann’s solution or 0.9% saline, but avoid too much chloride (i.e. 0.9% saline) if large quantities of fluid are required (risk of hyperchloraemic acidosis). Monitor response carefully – remember patients may need vasopressors to maintain blood pressure and reduce peripheral fluid losses.
Heart failure
Heart failure patients are prone to fluid overload and pulmonary oedema. Be attentive to their fluid balance and remember they may normally run hypotensive. If overload develops, start fluid restriction, furosemide, a low sodium diet, and record daily weights. There is no logic in giving furosemide together with fluids.
If a patient is at risk of LVF and has low SBP and urine output, you must examine the patient because there are two opposite explanations for this clinical picture:
Dehydration: they may simply be fluid deplete (treatment = fluids)
Worsening fluid overload: they may be fluid overloaded, which causes a low SBP, cardiorenal failure, and a low urine output (treatment = diuresis, which will reduce high venous pressure and improve LVF, increase SBP, and improve renal function and urine output)
Severe aortic stenosis
Patients with severe AS need adequate circulating volume to maintain preload, but be cautious because too much fluid too fast can cause flash pulmonary oedema (their high left ventricular end-diastolic pressure may be unable to accommodate extra fluid).
Liver disease
Excess Na+ may worsen ascites. Crystalloid use is fine acutely/for resuscitation, but try to avoid too much. Human albumin solution is a good alternative volume expander (e.g. 100ml 20% HAS).
Too much dextrose can also be problematic as it can worsen hyponatraemia (common in cirrhosis).
Acute kidney injury
Be cautious with potassium because they are at risk of hyperkalaemia.
Severe chronic kidney disease
Avoid excess fluid, sodium and potassium as the kidneys may not be able to excrete them
Alcoholic / risk of refeeding syndrome
Avoid dextrose where possible because it can precipitate re-feeding syndrome
If you need to give dextrose, give Pabrinex first because dextrose can precipitate Korsakoff syndrome
Brain haemorrhage/stroke
Avoid dextrose as this can cause osmotic haematoma swelling
Dextrose Destroys the brain if there’s a bleed!
Saline is best
Acute bleeding/trauma
In actively bleeding patients, fluid and blood product resuscitation is important; however, replacing fluid too aggressively may increase bleeding
For this reason, a less than normal blood pressure is often accepted – ‘permissive hypotension’
A 100kg patient is admitted pre-operatively for a liver lesion resection. He will be nil by mouth from midnight and the consultant has asked for maintenance IV fluids for 24 hours. His baseline U&Es are normal. What are the patients 24 hour requirements and what would be the most appropriate fluid prescription?
His fluid requirements will be:
H2O: 1.5ml/kg/hour = 150ml/h = 3.6L/24h
Na+: 1-2mmol/kg/day = 100-200mmol
K+: 0.5-1mmol/kg/day = 50-100mmol
Example prescription
1L dextrose-saline with 20mmol K+ at 150ml/h
1L dextrose-saline with 20mmol K+ at 150ml/h
1L dextrose-saline with 20mmol K+ at 150ml/h
500ml dextrose-saline at 150ml/h
This will give 105mmol Na+, 60mmol K+, and 3.5L fluid
A 42 year old has just had a bowel resection. The nurse has called for a fluid prescription. He will be allowed to eat and drink when able to but he is too drowsy currently. He has had U&Es: Na+ 136, K+ 4.6, Cr 70, Ur 5.5. He weighs 60kg. He appears euvolaemic. What would you prescribe and why?
Example prescription
1L dextrose-saline at 90ml/h
Reasoning
The patient will have had IV fluids to maintain euvolaemia during surgery so he will in effect need maintenance fluids until he can drink
He may had some insensible losses due to recent surgery but currently appears euvolaemic so maintenance would be adequate currently
His maintenance fluid rate will be 1.5ml/kg/hour = 90ml/h
He will have had a lot of sodium rich fluids in theatre so avoiding too much more sodium will prevent oedema, hyperchloraemic acidosis, increased kidney load, increased post-operative complications, and GI problems
Not including potassium in the fluid is preferred because of the cell lysis during surgery
Just prescribe 1L initially as the patient should be reassessed after each 1L to see if fluid is still required and assess the fluid rate and requirements if it is still required
A patient admitted with pyelonephritis has been having IV fluids which have run out and the nurse has asked for a further prescription. The patient has been having Hartmanns 1L at 8 hourly rate for the last 48 hours as she came in septic and vomiting. Her U&Es are normal. She is eating and drinking. She weighs 70kg. She appears euvolaemic clinically.
The patient does not need IV fluids as she is eating and drinking with no clear ongoing insensible losses and is euvolaemic.
A patient has been admitted to the emergency department due to profound vomiting due to gastroenteritis. She is hypotensive and tachycardic. U&Es show Na+ 132, K+ 2.9, Cr 155, Ur 16.8. Prescribe some initial IV fluids. She weighs 55kg and is clinically dehydrated.
Example prescription
500ml Hartmann’s STAT
Then 1L 0.9% sodium chloride with 40mmol KCl over 4 hours
Reasoning
The patient needs replacement of their pre-existing fluid deficit
An initial bolus of crystalloid 500ml is required, then reassessment to see if they need more
This patient also needs intravenous potassium replacement and the maximum rate that can be given peripherally is 10mmol/h. They require the maximum rate of potassium replacement given the severity of hypokalaemia. It should be rechecked after 1L with 40mmol to guide further replacement. It should be given in normal saline because the patient needs crystalloids to replace GI losses