2. Taylor francis 🧠: over 2500+ questions licenced from 18 text-books worth £191
3. Past examiners 🫁: Questions written by previous Medical School examiners
4. Track your performance 🏃♀️: QBank uses intelegent software to keep you on track
The reviews are in
★★★★★
6,893 users
Don't take our word for it
"The stations you provide are strikingly similar to those I came across during my medical school finals (some even verbatim!), and I have tried many other exam platforms. I'm truly grateful for your priceless support throughout my final couple of years at medical school!"
Raza Q 🇬🇧
"It has absolutely everything for medical school, so many histories with detailed differential diagnoses, how to approach emergencies, commonly prescribed drugs..every kind go examination you’ll ever need in osces"
John R 🇬🇧
"Thank you SO MUCH for the amazing educational resource. I’ve tried lots of platforms and books with mock OSCE stations and yours is by far and away the best I’ve tried"
Ed M 🇳🇿
"Get this right away. So helpful for OSCEs but also general clinical learning and understanding. Wish I had brought it sooner"
Emma W 🇬🇧
"Without a doubt, your platform outshines all other OSCE resources currently available. In all honesty, I can confidently attribute my success in securing a distinction in my finals to OSCEstop."
Harish K 🇬🇧
"OSCEstop distinguishes itself from many other platform banks by offering a wealth of questions that mimic the demanding and complex aspects of our finals. This platform played a crucial role in ensuring I was ready for the level of difficulty that awaited me in my final exams."
Membership includes access to all 4 parts of the site:
1. Learning 📖: All notes, viva questions, track progress
2. Stations 🏥: 10 years of past medical school stations. Includes: heart murmurs, ECGs, ABGs, CXR
3. Qbank 🧠: 2500+ questions from Taylor Francis books, complete MLA coverage
4. Conditions 🫀: all conditions mapped to MLA, progress tracking
The reviews are in
★★★★★
6,893 users
Don't take our word for it
"The stations you provide are strikingly similar to those I came across during my medical school finals (some even verbatim!), and I have tried many other exam platforms. I'm truly grateful for your priceless support throughout my final couple of years at medical school!"
Raza Q 🇬🇧
"It has absolutely everything for medical school, so many histories with detailed differential diagnoses, how to approach emergencies, commonly prescribed drugs..every kind go examination you’ll ever need in osces"
John R 🇬🇧
"Thank you SO MUCH for the amazing educational resource. I’ve tried lots of platforms and books with mock OSCE stations and yours is by far and away the best I’ve tried"
Ed M 🇳🇿
"Get this right away. So helpful for OSCEs but also general clinical learning and understanding. Wish I had brought it sooner"
Emma W 🇬🇧
"Without a doubt, your platform outshines all other OSCE resources currently available. In all honesty, I can confidently attribute my success in securing a distinction in my finals to OSCEstop."
Harish K 🇬🇧
"OSCEstop distinguishes itself from many other platform banks by offering a wealth of questions that mimic the demanding and complex aspects of our finals. This platform played a crucial role in ensuring I was ready for the level of difficulty that awaited me in my final exams."
The generic approach to musculoskeletal radiograph interpretation is covered separately. This is sufficient for most single bone radiographs. However, radiographs of many joints/areas require a specific approach to interpretation or have specific signs which need to be looked for within the ABCS approach – these are outlined here.
Facial bones
Identify zygoma (stool) and look for fractures of its 4 legs:
Zygomatic arch – if you imagine the zygoma as an elephant’s head, this leg looks like an its trunk on a radiograph
Frontal process of zygoma
Orbital floor
Lateral wall of maxillary antrum
Soft tissue signs indicating a fracture (working downwards)
Black eyebrow sign – black eyebrow like shadow across top of orbit (air in orbit from sinus, usually due to orbital blow-out fracture)
Teardrop sign – dark shadow at the top of the maxillary antrum (soft tissue herniation of orbital contents from orbital blow-out fracture)
Fluid level – in maxillary antrum (blood from fracture)
Common facial bone pathology
Nasal bone fracture: commonly due to punch injury; may not be seen on radiographs and X-rays are not performed to specifically look for it as it does not change management; look up the patient’s nose to exclude a septal haematoma!
Mandible fracture: commonly due to punch injury; use an OPG X-ray to look for it, not a facial bone X-ray
Zygomatic arch fracture
Orbital floor fracture
‘Tripod’ fracture: fractures of all 4 ‘legs’ of the zygoma due to major trauma – should really be called a quadripod fracture
Cervical spine
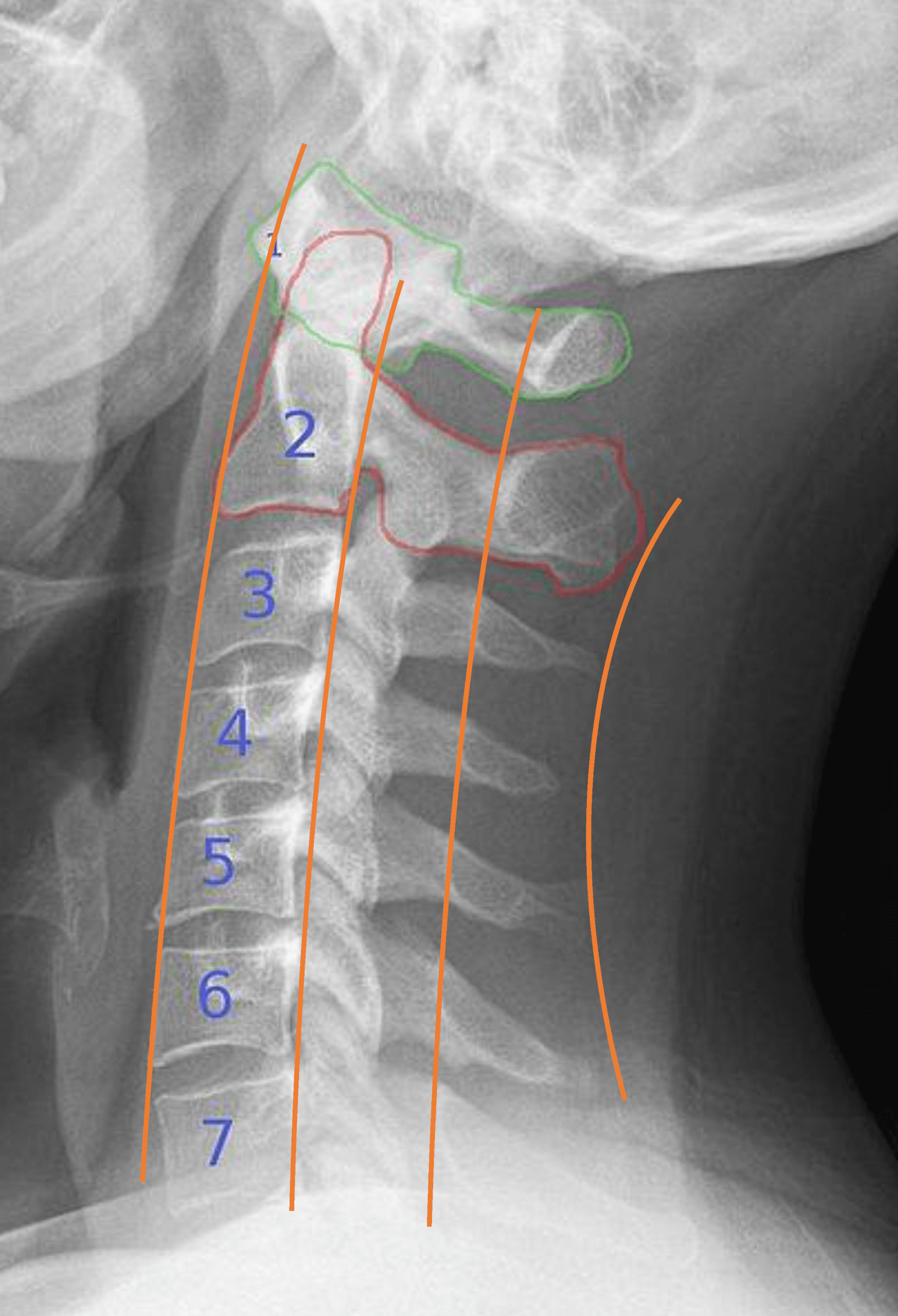
Lateral view (ABCS)
First check Adequacy: Need to see skull base and C7/T1 disc space (if not, get swimmer’s view)
Alignment
Alignment arcs (look for smooth curves)
Anterior vertebral body line
Posterior vertebral body line
Spinolaminar line (anterior edges of spinous processes)
Posterior spinous line (posterior edges of spinous processes)
Lateral cervical spine alignment arcs
Bones
Peg of C2 sticking up
Should be smooth and flat
Atlanto-axial space should be <5mm in adults or <3mm in children (the space in front of the peg, before the posterior part of C1 tubercle)
Harris ring of C2 integrity (formed by: body of C2 anteriorly and posteriorly, and borders of the pedicles superiorly and inferiorly)
Trace around each vertebral body to look for fractures
Cartilage
Equal gaps between vertebral bodies
Soft tissues
Anterior para-spinal soft tissue width (line in front of vertebral bodies)
C1-4 = < a third vertebral body width
C5-7 = < whole vertebral body width
AP view
Spinous processes
Alignment in straight line (may need to go down middle of bifid processes)
Distance apart
PEG view
Outline bones and check gaps
Peg
C2 attached
C1’s lateral masses and their alignment with the peg and C2’s lateral masses
Common C-spine pathology
C1
Jefferson fracture: multiple fractures at different points in C1 ring due to a compressing vertical force
Rupture of transverse ligament of C1 causing C2 subluxation: revealed by asymmetry of gaps between peg and C1’s lateral masses on peg view, and increased atlanto-axial space on lateral view
C2
Base of peg fracture
Hangman’s fracture: fractures of both pedicles of C2 due to hyperextension injury e.g. hanging or head striking dashboard in RTA
C3-7
Spinous process fracture
Vertebral body compression fracture
Burst fracture: comminution of a vertebral body due to vertical compression force
Extension teardrop fracture: avulsion of anteroinferior vertebral body corner due to sudden pull of anterior longitudinal ligament during forced extension
Flexion teardrop fracture: compression anterior vertebral body with anteroinferior vertebral body fragment detachment due to extreme flexion and axial loading
Anterior subluxation: disruption of alignment arcs due to flexion-rotation injury
Unilateral facet joint dislocation: difficult to see – spinous processes may not be aligned on AP view and may be subluxation on lateral view
Note, up to 10% of fractures may not be visible on C-spine radiographs. If you are still clinically suspicious of a fracture, consider CT
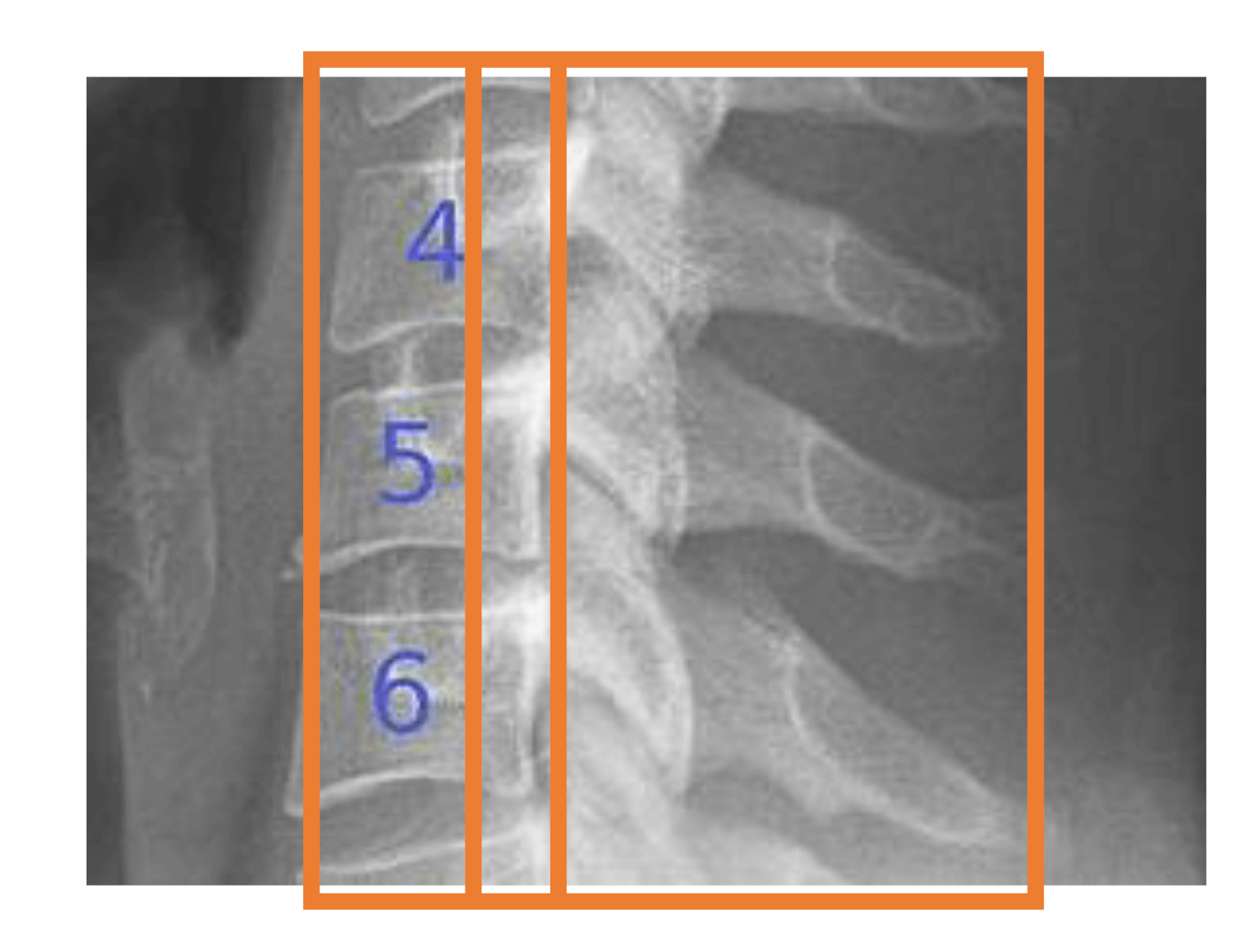
Thoracic and lumbar spine
Lateral view (ABCS)
Alignment
Alignment arcs (look for smooth curves)
Anterior vertebral body line
Posterior vertebral body line
Bones
Trace around each vertebral body to look for fractures
Loss of vertebral height/wedging
Cartilage
Gaps between vertebral bodies (disc spaces gradually increase, except for L5/S1 which is slightly smaller)
Soft tissues
Anterior para-spinal soft tissue width (line in front of vertebral bodies)
AP view
Alignment of spinous processes and lateral sides of vertebral bodies (arcs)
Pedicles – check for equal distances between
Transverse processes – look for fractures
Paraspinal soft tissue lines in thoracic spine (bulging may be paraspinal haematoma due to a fracture)
Spine stability
When an injury is detected, it must be classified as stable or unstable
The spine is formed by ‘3 columns’ – if 2 or more are disrupted, the injury is unstable
Anterior column = anterior longitudinal ligament, anterior part of annulus, anterior two thirds of vertebral body
Middle column = posterior longitudinal ligament, posterior part of annulus, posterior margin of vertebral body
Osteoporotic compression fracture: most common by far; may be clinically silent
Wedge compression fracture: compression of anterior portion of vertebral body due to flexion injury
Transverse process fractures: caused by rotation or extreme lateral bending
Burst fracture: comminution of a vertebral body due to vertical compression force e.g. landing on feet from high fall
Fracture-dislocation injury: a vertebral fracture with subluxation/dislocation of the vertebra
Chance fracture: anterior vertebral body compression with transverse fracture of the body, fracture of the posterior part of the body and fracture of the posterior elements of the vertebra (e.g. spinous process) due to violent forward flexion shearing injury e.g. RTA
Superior border of humeral head should have a walking stick appearance (lost in posterior dislocation – looks like a lightbulb)
Acromioclavicular joint – inferior corticies of clavicle should align with acromion process
Coracoclavicular joint – distance between coracoid and clavicle should be <1.3cm
Bones – outline all bones to look for fractures
Humerus head and neck
Glenoid margin
Clavicle
Body or neck of scapula
Apical oblique view
Alignment of humeral head and glenoid (glenoid looks like a triangle, the centre of which should be immediately adjacent to centre of humeral head)
Look for fractures of humeral head/neck and glenoid margin
Scapula Y view (lateral)
Alignment of humeral head and glenoid (humeral head should be in the centre of the glenoid which is in the middle of the Y shape formed by the scapula’s blade + acromium + coracoid)
Note: on this lateral view, anterior is towards the ribs and posterior is away from the ribs
Common shoulder pathology
Anterior dislocation of glenohumeral joint: seen on AP view as humeral head lying directly below coracoid process; associated fractures:
Hill-Sachs lesion – compression fracture of posterolateral aspect of humeral head
Bankart lesion – anterior lip of glenoid breaks off
Avulsion fracture of supraspinatus origin
Humeral head fracture e.g. greater tuberosity
Posterior dislocation of glenohumeral joint (rare, but often occurs during epileptic fit): humeral head looks like lightbulb on AP view (loss of walking stick appearance); seen clearly on apical oblique and scapula Y views where humeral head is posterior to glenoid
Fracture of greater tuberosity of humerus
Proximal humeral fracture
Clavicle fracture: occur due to fall on shoulder or out-stretched hand or direct trauma
Acromioclavicular joint dislocation/subluxation
Elbow
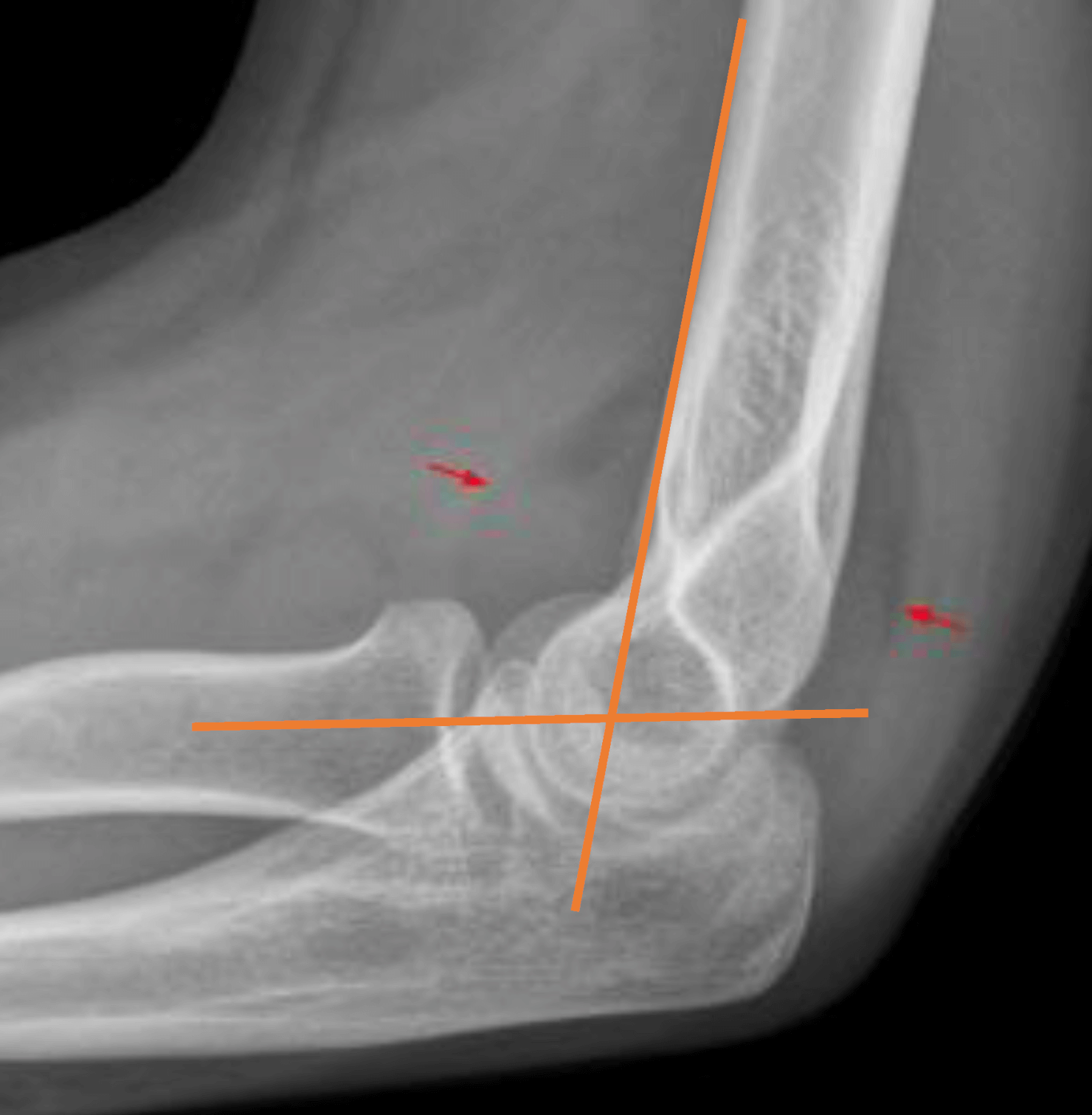
Lateral view
Alignment
Radiocapitellar line (can also view on AP view) – line in the centre of the long axis of the proximal 2-3cm of radius should transect the capitellum circle (if not, there is dislocation of radial head)
Anterior humeral line (in children to rule out subtle supracondylar fracture) – should transect the capitellum circle, with at least one third of the circle anterior to the line
Elbow alignment
Elbow fat pads (seen as dark streaks closely related to anterior and posterior part distal humerus)
Presence
Anterior – can be normal
Posterior – abnormal because the fat is usually hidden in the olecranon fossa, presence indicates a fracture
Displacement – indicates a fracture (see example in image)
Lateral and AP views
Bones – trace all bones looking for fractures (look closely at radial head and neck cortex)
Ossification centres in children
Accumulate in sequence below (CRITOL) – check they are normal and appear by dates below
Capitellum = 2y (part of humerus that articulates with radius)
Radial head = 4y
Internal (medial) epicondyle = 6y
Trochlea = 8y (part of humerus that articulates with ulna)
Olecranon = 10y
Lateral epicondyle = 12y
Common elbow pathology
Fracture of head or neck of radius (most adults)
Olecranon fracture
MonteggiA: fractuA of ulnA + dislocation of radial head (don’t confuse with Galeazzi below)
In children
Supracondylar fracture (most children): assess using anterior humeral line; high risk of vascular damage
Avulsion of epicondyles
Wrist and distal forearm
PA view
Alignment
Radial articularsurface should lie distal to ulna
Scapho-lunatedistance should be <2mm wide (increased if ligamentous injury – causes chronic wrist pain)
Bones – trace all bones looking for fractures (look closely at radial articular surface, ulna styloid process, scaphoid, and any cortical angulation or bulges in children)
Lateral view
Alignment
Normal apple-in-cup (on saucer) alignment of radius, lunate and capitate (image below)
Palmar tilt of radial articular surface should be 2-20˚ (may be impacted fracture if not)
Bones – specifically:
Dorsal cortex of distal radius
Bone fragment posterior to carpal bones (triquetral fracture)
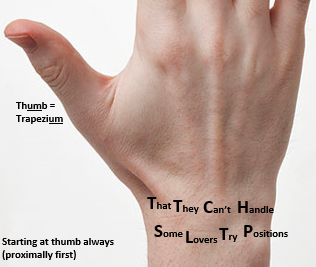
Carpal bones mnemonic
Carpal bones radiographic appearance
Common wrist/forearm pathology
Distal radius fracture
Colles’ fracture: distal radius fracture with dorsal angulation
Smith’s fracture: distal radius fracture with volar angulation
Scaphoid fracture: scaphoid views should be requested if suspected (clinical signs: 1. anatomical snuffbox tenderness, 2. scaphoid tubercle tenderness, 3. thumb telescoping tenderness) – however, fractures are often not visible on X-rays until 10 days, so if clinically suspicious treat and re-X-ray in 10 days; scaphoid fractures are important because of the retrograde blood supply and risk of avascular necrosis
Triquetral fracture: bone fragment posterior to carpal bones indicated triquetral avulsion fracture
Lunate dislocation: cup (lunate) of the apple-in-cup dislocates anteriorly leaving other bones in place
Perilunate dislocation: cup (lunate) is in line but the apple (capitate) and all other carpals are displaced posteriorly
Greenstick fracture (in children): revealed by slight angulation of bone cortex
Torus fracture (in children): revealed by slight bulge of bone cortex
Distal radius growth plate fracture (in children)
Galeazzi: fracture of radius + dislocation of distal ulna (GFR = Galeazzi Fractured Radius – don’t confuse with Monteggia above)
Pelvis and hip
AP view
Alignment
Shenton’s line – smooth imaginary curve joining curve of inferomedial neck of femur and curve of inferior border of superior pubic ramus (disruption indicates a neck of femur fracture)
Femoral head alignment with acetabulum(can dislocate any way inc medially)
Symphysis pubis – width should be <5mm and superior pubic rami bones should align
Sacro-iliac joint widths should be equal
Bones
Proximal femur(s)
Acetabulum (look through the femoral head)
Large ring – trace inner and outer parts of pelvic ring
2 small rings – trace obturator foramen and outer pubic/ischial bones
Sacral foramina (compare sides)
Lateral hip
Specifically check
Neck of femur
Trochanteric region
Synchondroses and apophyses in children/adolescents
Check they are the same on each side
Synchondroses are the cartilaginous connections between the ischial and pubic bones in children before they fuse
Apophyses are small secondary bones (connected to main bones via growth plates) to which muscles attach. This makes them prone to avulsion. Most are seen on radiographs between 13-15 years of age, after which they begin to fuse (takes ~ 5 years)
Iliac crest (abdominal muscles)
ASIS (sartorius/tensor fasciae latae)
AIIS (rectus femoris)
Ischial tuberosity (hamstrings)
Greater trochanter (gluteus muscles)
Lesser trochanter (iliopsoas)
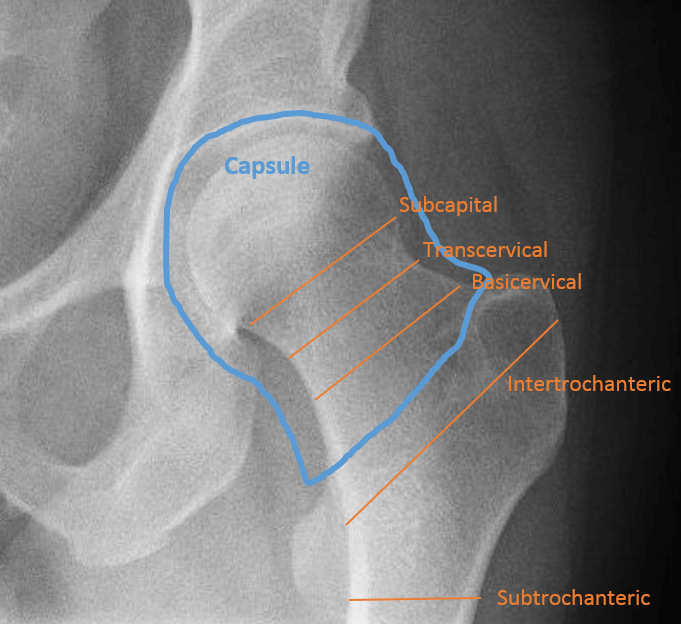
Neck of femur fractures
Elderly patient after fall; may be a while line (impacted) or black line (displaced); classified as per image; management:
Intracapsular (risk of avascular necrosis)
Displaced >60y → THR if active and with-it, hemiarthroplasty if not
<60y or undisplaced → try cannulated screws
Extracapsular
Intertrochanteric → dynamic hip screw or gamma nail
Subtrochanteric → intra-medullary nail
Other common hip/pelvis pathology
Pubic rami fracture: elderly patient after fall
Acetabular fracture: in major trauma or femoral head dislocation; bone fragments may be seen
Avulsion fractures: bone at sites of tendon insertion can be ripped off occur during sports injuries
Femoral head dislocation: occurs commonly after total hip replacement and in major trauma
Children and adolescents
Perthe’s disease: 5-10 years; signified by increased density and decrease in size of epiphysis
Slipped upper femoral epiphysis (SUFE): 10-15 years; seen best on lateral radiograph
Femoral and iliac apophyseal avulsions: occur due to sudden muscle contraction in adolescence (most are ASIS/AIIS/ischial tuberosity)
Vertical lines drawn from the most medial and lateral parts of the femoral epicondyles should have <5mm of the adjacent tibial condyles outside (if more, may be tibial plateau fracture)
Bones
Femur – especially the condylar surfaces
Tibia – look closely at each tibial plateau (should be very smooth), their subchondral bone and the intercondylar eminence
Fibula – head and neck
Patella – look through femur
Bone fragments anywhere
Lateral view
Patella position – the distance from the patella to the tibial tubercle should be the length of the patella itself ± 20% (may be increased in patella tendon rupture)
Articular surfaces and the femur and patella, and for any bone fragments
Suprapatella bursa (seen as longitudinal dark shadow superior to the patella, between prefemoral fat and suprapatellar fat)
AP width – should be <5mm wide (called the ‘suprapatellar strip’ if normal, indicates joint effusion if increased)
Fat-fluid level in suprapatella bursa (indicates intra-articular fracture because the fat is from bone marrow)
In children, also look for
Growth plates of femur, tibia, fibula – look for epiphyseal fracture
Cortex of femur and tibia for any cortical angulation (greenstick fracture) or bulges (torus fracture)
Femoral condylar surfaces – look for osteochondral lesion or fracture
Common knee pathology
Tibial plateau fracture: may be subtle; commonly seen as lateral tibial plateau depression following traumatic compression by lateral femoral condyle; can be classified using Schatzker classification
Patella body fracture: caused by direct blow
Neck of fibula fracture: ensure the common peroneal nerve function is tested
Patella dislocation: usually dislocates laterally
Patella tendon rupture: high patella
ACL/PCL avulsion fractures: look for bone fragments from the tibial intercondylar eminence within the joint
Segond fracture: avulsion of a fragment from the lateral tibial condyle by the lateral collateral ligament
Stress fracture of tibia: appears as sclerotic band
Ankle (& hindfoot)
AP mortice
Alignment
Tibia and fibula (increased distance indicates tibiofibular interosseous membrane rupture)
Should overlap distally
Distance between them should be <6mm (measured 1cm proximally to lateral tibial articular surface)
Tibiotalar joint width <4mm
Bones
Talus dome and medial and lateral tubercles
Malleoli
Growth plates (in children)
Lateral view
Alignment
Bohler’s angle of calcaneum – draw a line from highest anterior point to the highest mid-point, then draw a second line from the highest posterior point to the highest mid-point – the acute angle between the lines should be >30˚ (decreased angle suggests calcaneal fracture)
Talonavicular joint
Bones
Tibia
Fibula
Talus – especially neck
Calcaneum
5th metatarsal base
Common ankle pathology
Calcaneus fracture: occurs after fall from height; if suspected, an axial (calcaneal) view should be requested
Weber B = at ankle joint (syndesmosis intact or partially torn)
Weber C = above ankle joint (syndesmosis disrupted)
Medial malleolus fracture
Bimalleolar fracture: fracture of lateral malleolus and medial malleolus
Trimalleolar fracture: fracture of lateral malleolus, medial malleolus and posterior lip of tibia
Base of 5th metatarsal fracutre: forced foot inversion pulls peroneus brevis tendon which avulses base of 5th metatarsal
Distal tibia growth plate fracture in children
Tibiofibular interosseous membrane (syndesmosis) tear: revealed by increased distance between the distal tibia and fibula
Foot (midfoot and forefoot)
AP view
Alignment
Lisfranc joint (5 tarsometatarsal joints held by Lisfranc ligament complex)
2nd metatarsal base held in mortice by 3 cuneiforms
Medial side of 2nd metatarsal base should align with medial side of intermediate cuneiform
Bones
Metatarsal shafts
Phalangeal shafts
Oblique view
Alignment
Lisfranc joint
Medial side of 3rd metatarsal base should align with the lateral cuneiform
Hindfoot (calcaneus and talus) articulations with midfoot (cuboid, navicular, cuneiforms)
Bones
Metatarsal shafts
Hindfoot bones
Common foot pathology
Phalanx fractures
Metatarsal fractures
Metatarsal stress fractures
Base of 5th metatarsal fracture: forced foot inversion pulls peroneus brevis tendon which avulses base of 5th metatarsal
Lisfranc injury: low impact strain
Lisfanc subluxation: high impact injury resulting in subluxation at a Lisfranc joint
Salter-Harris grading of growth plate fractures in children
Children’s long bones will have growth plates at either end. Fractures can involve these growth plates and are graded by the Salter-Harris classification (SALTR):
Grade I = Separated (fracture straight across growth plate, separating diaphysis from epiphysis)
Grade II = Above (fracture part across growth plate and part going up into diaphysis)
Grade III = beLow (fracture part across growth plate and part going down into epiphysis)
Grade IV = Through (fracture at an angle to growth plate goes right through it)
Grade V = Rammed together (impaction of diaphysis and epiphysis)
Digital image manipulation tips
Increase the contrast
Click ‘sharpen edges’
If you don’t zoom, you will get sued!
To find fractures, trace closely around around the cortex, but also look at the continuity of the trabeculae
Image references
C-spine X-rays (edited with additional lines): 2010 Hellerhoff. licensed under the Creative Commons Attribution-Share Alike 3.0 Unported license (https://creativecommons.org/licenses/by-sa/3.0/deed.en). Sourced from: https://commons.wikimedia.org/wiki/File:HWS_seitlich_Annotation.jpg
Elbox X-ray (edited with additional lines): Hellerhoff. Licensed under the Creative Commons Attribution-Share Alike 3.0 Unported license (https://creativecommons.org/licenses/by-sa/3.0/). Sourced from: https://wikem.org/wiki/File:Ant_and_post_fat_pad.png#filelinks