2. Taylor francis 🧠: over 2500+ questions licenced from 18 text-books worth £191
3. Past examiners 🫁: Questions written by previous Medical School examiners
4. Track your performance 🏃♀️: QBank uses intelegent software to keep you on track
The reviews are in
★★★★★
6,893 users
Don't take our word for it
"The stations you provide are strikingly similar to those I came across during my medical school finals (some even verbatim!), and I have tried many other exam platforms. I'm truly grateful for your priceless support throughout my final couple of years at medical school!"
Raza Q 🇬🇧
"It has absolutely everything for medical school, so many histories with detailed differential diagnoses, how to approach emergencies, commonly prescribed drugs..every kind go examination you’ll ever need in osces"
John R 🇬🇧
"Thank you SO MUCH for the amazing educational resource. I’ve tried lots of platforms and books with mock OSCE stations and yours is by far and away the best I’ve tried"
Ed M 🇳🇿
"Get this right away. So helpful for OSCEs but also general clinical learning and understanding. Wish I had brought it sooner"
Emma W 🇬🇧
"Without a doubt, your platform outshines all other OSCE resources currently available. In all honesty, I can confidently attribute my success in securing a distinction in my finals to OSCEstop."
Harish K 🇬🇧
"OSCEstop distinguishes itself from many other platform banks by offering a wealth of questions that mimic the demanding and complex aspects of our finals. This platform played a crucial role in ensuring I was ready for the level of difficulty that awaited me in my final exams."
Membership includes access to all 4 parts of the site:
1. Learning 📖: All notes, viva questions, track progress
2. Stations 🏥: 10 years of past medical school stations. Includes: heart murmurs, ECGs, ABGs, CXR
3. Qbank 🧠: 2500+ questions from Taylor Francis books, complete MLA coverage
4. Conditions 🫀: all conditions mapped to MLA, progress tracking
The reviews are in
★★★★★
6,893 users
Don't take our word for it
"The stations you provide are strikingly similar to those I came across during my medical school finals (some even verbatim!), and I have tried many other exam platforms. I'm truly grateful for your priceless support throughout my final couple of years at medical school!"
Raza Q 🇬🇧
"It has absolutely everything for medical school, so many histories with detailed differential diagnoses, how to approach emergencies, commonly prescribed drugs..every kind go examination you’ll ever need in osces"
John R 🇬🇧
"Thank you SO MUCH for the amazing educational resource. I’ve tried lots of platforms and books with mock OSCE stations and yours is by far and away the best I’ve tried"
Ed M 🇳🇿
"Get this right away. So helpful for OSCEs but also general clinical learning and understanding. Wish I had brought it sooner"
Emma W 🇬🇧
"Without a doubt, your platform outshines all other OSCE resources currently available. In all honesty, I can confidently attribute my success in securing a distinction in my finals to OSCEstop."
Harish K 🇬🇧
"OSCEstop distinguishes itself from many other platform banks by offering a wealth of questions that mimic the demanding and complex aspects of our finals. This platform played a crucial role in ensuring I was ready for the level of difficulty that awaited me in my final exams."
Please note OSCEstop content is for educational purposes only and not intended to inform clinical practice. OSCEstop and authors take no responsibility for errors or the use of any information displayed.
When to use an ABCDE assessment
This protocol should be used for critically ill patients. For example those with very unstable observations or reduced GCS.
Airway
Assessment
It’s patent if the patient can talk and breathing is not noisy
It’s not if: there are secretions; the patient has aspirated; is snoring/ GCS<8; or stridor is present
Look inside the mouth – are there any obstructions? Is there mucosal oedema?
Management
Consider:
Remove dentures/debris (Magill forceps are in crash trolley)
Suction
Airway opening manoeuvres (e.g. jaw-thrust or head-tilt/chin lift)
Recovery position if vomiting/aspiration risk
Oropharyngeal / nasopharyngeal airways
Intubation (if GCS <8)
Cricothyroidotomy may be required in upper airway obstruction where intubation is not possible
Treat cause
Treat any evident causes (e.g. anaphylaxis, foreign body)
WARNING: take care if COPD (unless they are in respiratory distress/critically unwell and need high-flow oxygen, start at 24-28% venturi and aim for sats 88-92%. Titrate to ABG results. See notes on oxygen therapy.)
Consider non-invasive or invasive ventilation if hypoxaemic, or hypercapnic respiratory acidosis despite maximal therapy
If respiratory effort is inadequate, it must be supported (e.g. ventilate with bag-mask)
Auscultate heart, check JVP and look for signs of fluid overload
Assess fluid balance and organ perfusion (IN e.g. fluids, intake; OUT e.g. catheter/urine, drains, vomit)
Tests
Place wide-bore IV Cannula and take bloods (also do VBG for fast results if ABG not required)
Apply 3-lead cardiac monitoring
ECG (if any concern)
Catheter and fluid balance monitoring (if hypotensive/unwell)
Management
Hypotension
Lay supine and elevate legs
Fluid challenge = 500ml 0.9% saline/Hartmann’s solution STAT and monitor response by HR, BP and UO (see prescribing notes on fluids)
WARNING: take care if significant heart failure history (use 250ml if they need it)
Shock
2 large bore IV cannulas
Fluid challenge = 1L 0.9% saline/Hartmann’s solution STAT
Replace blood with blood (can give O negative or urgent typing takes 15 minutes). In massive blood loss, call 2222/lab and activate the massive blood loss protocol to get packed red cells + FFP ± platelets
Further management– use clinical judgement and assessment of fluid status
Respond fully: consider maintenance fluids
Responds but BP falls again: may require further fluids (adequate resuscitation depends on patient and degree of deficit but may be around 20-30ml/kg)
No response: patient may be fluid overloaded/in cardiogenic shock (avoid further fluids) or very deplete (requiring further fluids)
Escalation
If patient is hypotensive and overloaded, they need inotropes
If patient is still hypotensive despite adequate fluid resuscitation (20-30ml/kg), they need vasopressors
Refer to other specialty if indicated, for example:
Medical registrar: medical problems
Endoscopist on call: upper GI bleeding
Surgical registrar: surgical problems and bleeding
Cardiology registrar: MI/arrhythmia
Gynaecological registrar: ruptured ectopic
Intensive/high-dependency care registrar: if patient may need higher level of care / airway concerns
Document in patient’s notes
Document with a brief case summary, ABCDE headings with findings and management
Review patient and results as necessary
Test your knowledge
Scenario 1
You are reviewing a breathless patient on the acute medical unit waiting to be clerked with known COPD, admitted with breathlessness. You undertake an A-E assessment. His airway is patent. His respiratory rate is 32, and the nurse has put him on 35% oxygen via Venturi mask as he had low oxygen saturations. His chest sounds very wheezy. You perform an arterial blood gas.
The patient has now had all of the treatment you prescribed and you repeat an ABG. This shows ongoing type 2 respiratory failure with acidosis. What would you do now?
You are in the resuscitation area of the emergency department. A male patient is brought in with a low GCS. The patient’s name, details and medical history are unknown. You immediately undertake a rapid A-E assessment:
A: talking but confused
B: RR 8, Sats 91% on air, chest sounds clear
C: BP 122/80, HR 69, capillary refill <2 seconds, nurses unable to succeed in establishing IV access
D: eyes open in response to pain; pupils pinpoint; withdraws from pain but does not follow commands; confused speech; capillary glucose 5.8
E: unkempt; no rashes or bleeding; needle marks noted in groins
You are asked to see a 49 year old female patient on a surgical ward who has been admitted for an elective Whipple’s procedure for pancreatic cancer. The procedure was undertaken 6 days previously. She has had no other medical problems previously. The nurse has asked you to see the patient because of a high NEWS score. Observations are as follows:
HR 145, BP 98/68, RR 22, Sats 90% on air (improved to 95% on 4L nasal oxygen), temperature 38.2, GCS 15
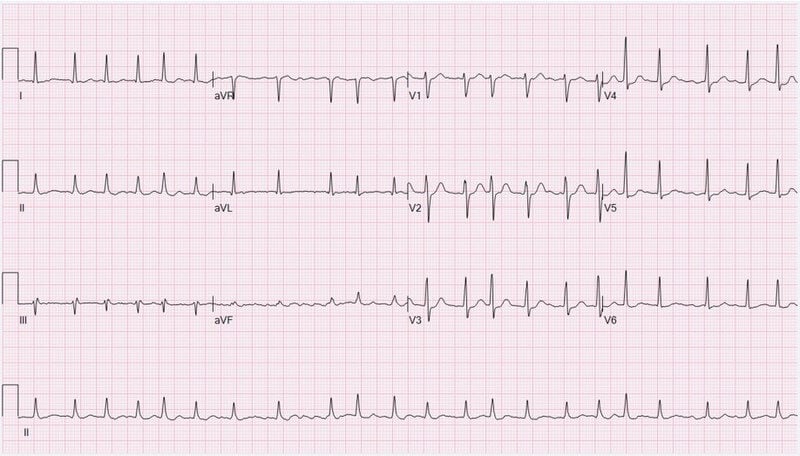
The nurse has already performed an ECG prior to your arrival. There was a previous normal pre-op ECG 8 days ago.
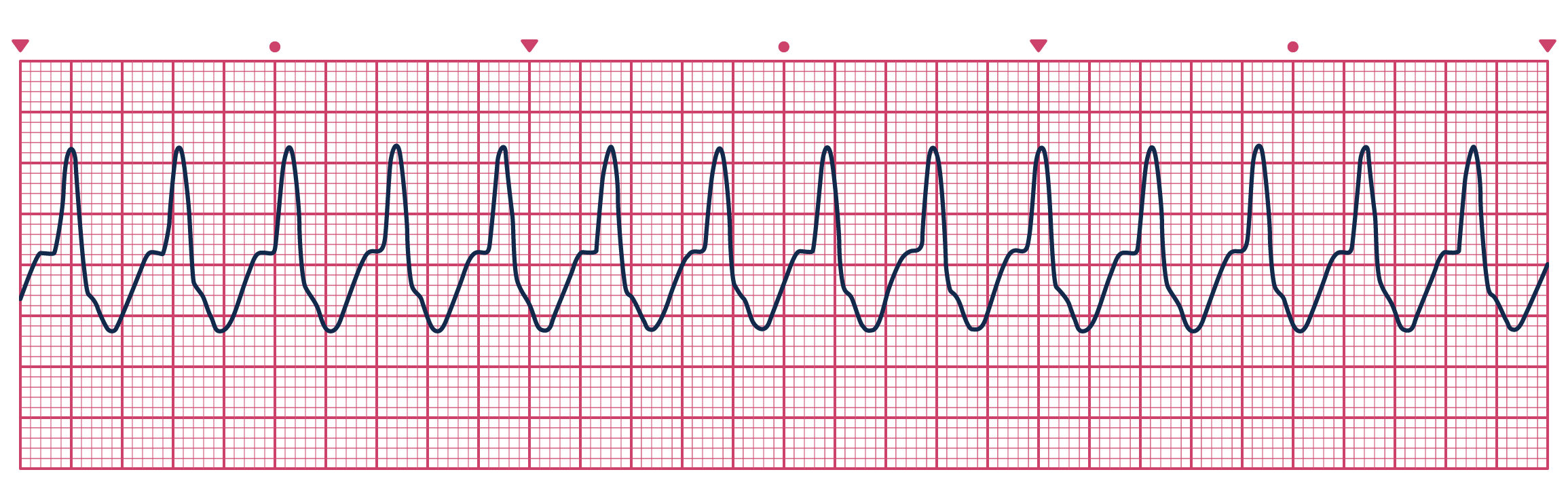
ECG (click to enlarge
You examine the patient and hear coarse crepitations in the left lower zone posteriorly. Heart sounds are normal but irregular. Mucus membranes look dry. You are unable to see the JVP. There is no peripheral oedema or rashes. The surgical wound is clean.