2. Taylor francis 🧠: over 2500+ questions licenced from 18 text-books worth £191
3. Past examiners 🫁: Questions written by previous Medical School examiners
4. Track your performance 🏃♀️: QBank uses intelegent software to keep you on track
The reviews are in
★★★★★
6,893 users
Don't take our word for it
"The stations you provide are strikingly similar to those I came across during my medical school finals (some even verbatim!), and I have tried many other exam platforms. I'm truly grateful for your priceless support throughout my final couple of years at medical school!"
Raza Q 🇬🇧
"It has absolutely everything for medical school, so many histories with detailed differential diagnoses, how to approach emergencies, commonly prescribed drugs..every kind go examination you’ll ever need in osces"
John R 🇬🇧
"Thank you SO MUCH for the amazing educational resource. I’ve tried lots of platforms and books with mock OSCE stations and yours is by far and away the best I’ve tried"
Ed M 🇳🇿
"Get this right away. So helpful for OSCEs but also general clinical learning and understanding. Wish I had brought it sooner"
Emma W 🇬🇧
"Without a doubt, your platform outshines all other OSCE resources currently available. In all honesty, I can confidently attribute my success in securing a distinction in my finals to OSCEstop."
Harish K 🇬🇧
"OSCEstop distinguishes itself from many other platform banks by offering a wealth of questions that mimic the demanding and complex aspects of our finals. This platform played a crucial role in ensuring I was ready for the level of difficulty that awaited me in my final exams."
Membership includes access to all 4 parts of the site:
1. Learning 📖: All notes, viva questions, track progress
2. Stations 🏥: 10 years of past medical school stations. Includes: heart murmurs, ECGs, ABGs, CXR
3. Qbank 🧠: 2500+ questions from Taylor Francis books, complete MLA coverage
4. Conditions 🫀: all conditions mapped to MLA, progress tracking
The reviews are in
★★★★★
6,893 users
Don't take our word for it
"The stations you provide are strikingly similar to those I came across during my medical school finals (some even verbatim!), and I have tried many other exam platforms. I'm truly grateful for your priceless support throughout my final couple of years at medical school!"
Raza Q 🇬🇧
"It has absolutely everything for medical school, so many histories with detailed differential diagnoses, how to approach emergencies, commonly prescribed drugs..every kind go examination you’ll ever need in osces"
John R 🇬🇧
"Thank you SO MUCH for the amazing educational resource. I’ve tried lots of platforms and books with mock OSCE stations and yours is by far and away the best I’ve tried"
Ed M 🇳🇿
"Get this right away. So helpful for OSCEs but also general clinical learning and understanding. Wish I had brought it sooner"
Emma W 🇬🇧
"Without a doubt, your platform outshines all other OSCE resources currently available. In all honesty, I can confidently attribute my success in securing a distinction in my finals to OSCEstop."
Harish K 🇬🇧
"OSCEstop distinguishes itself from many other platform banks by offering a wealth of questions that mimic the demanding and complex aspects of our finals. This platform played a crucial role in ensuring I was ready for the level of difficulty that awaited me in my final exams."
By the time you get to the sensory exam you should know what you are expecting to find and use it to confirm or narrow down differentials (see neurology differentials).
Introduction
Wash hands
Introduce self
Ask Patient’s name, DOB and what they like to be called
Explain examination and obtain consent
Expose patient’s legs (to underwear or shorts)
Inspection
General inspection
Look at the patient in general: posture, habitus, other signs of neurological conditions (e.g. hypomimia, facial muscle wasting)
Look around bed, for example you may see: mobility aids, orthoses
Gait – first ask if they can walk and if they need assistance/aids
Normal walking
Heel-to-toe walking if stable (ataxia = cerebellar pathology)
Stand on heels and then toes (tests distal power)
Romberg’s test (only if steady): ask patient to close eyes and assess their stability (reduced stability = sensory ataxia due to proprioceptive deficit)
Local inspection – look closely at the legs
Involuntary movements e.g.tremors
Muscles: muscle wasting – in general and then look closely for plantar foot wasting and for dorsal foot guttering(LMN lesion); fasciculations(LMN lesion); associated bony deformity (e.g. pes cavus)
Tone: patient should lie relaxed with legs flat. With one hand either side of the knee, roll each leg from side to side
↑tone, i.e. foot remains in line with knee = UMN lesion
↓ tone = LMN lesion
Spasticity: place hand under the patient’s knee and briskly lift it up (spasticity, i.e. foot kicks out involuntarily = UMN lesion)
Clonus: hold the sole of the patient’s foot in one hand, and elevate it while holding their ipsilateral knee flexed in the other hand. Forcefully flex the ankle a few times quickly, and then hold it firmly in the flexed position. Feel for involuntary, rhythmic beats of gastrocnemius contraction (>5 beats = UMN lesion).
Power
Test one joint at a time and compare sides. Always support the joint being tested with one hand (use it as a lever). Use all your strength!
Hip flexion (L2/L3)
Patient should raise their leg off the bed with knee fully extended. Stabilise contralateral hip joint with one hand and push down on the quadriceps just above the knee of the raised leg. ‘Don’t let me push your leg down.’
Hip extension (L4/L5)
With the same leg still raised to about 30˚, stabilise the ipsilateral hip joint with one hand and hold the underside of the patient’s knee with the other hand. ‘Push my hand down into the bed.’
Knee extension (L3/L4)
With the patient’s knee flexed to about 90˚, stabilise the joint with one hand and hold the anterior side of their ankle with your other hand and try to push it towards them. ‘Try and kick your leg out. Don’t let me push it towards you.’
Knee flexion (L5/S1)
In the same position, but holding the posterior side of their ankle, try and pull it away. ‘Try and pull your heel towards your bottom. Don’t let me pull it away.’
Ankle dorsiflexion (L4/L5)
With their leg straight on the bed and their ankle actively dorsiflexed, stabilise the ankle with one hand. Make a fist with your other and use the dorsal side of your fist to try and push the patient’s foot downwards. ‘Point your foot up towards your head. Don’t let me push it down.’
Ankle plantar-flexion (S1/S2)
With their leg straight on the bed and their ankle actively plantar-flexed, try to pull it up with your fingers around the ball of the patient’s foot. ‘Point your foot downwards towards the bottom of the bed. Don’t let me pull it up.’
Big toe extension (purely L5)
With their big toe actively flexed, isolate the toe’s metatarsophalangeal joint with one hand and try to push it down with the index and middle fingers of your other hand. ‘Point your big toe up towards your head. Don’t let me push it down.’
MRC power grades
5 = full power
4 = some resistance
3 = GRAVITY
2 = gravity eliminated
1 = flicker of muscle contraction
0 = nothing.
Reflexes
Hold the tendon hammer by the end of the plastic rod to make a pendulum-like swing. Ensure the patient is fully relaxed. If you cannot elicit a reflex, ask them to close their eyes and grit their teeth when you strike the tendon. Reflexes may be brisk, normal, reduced or absent.
Patellar (L3/4)
Patellar = L3, 4 kick the door
With the knee relaxed in passive flexion (hold it up with your left wrist under the patient’s knee), locate the tibial tuberosity and inferior border of the patella
Strike the patellar tendon that lies between these
Ankle (S1/2)
Ankle = S1, 2 in the shoe
Externally rotate the patient’s leg and flex their knee (so their lower leg rests over their contralateral shin)
Hold their foot with your left hand and gently dorsiflex their ankle
Strike the Achilles tendon with the hammer in your right hand
NB: to test their left ankle reflex, move to the base of the bed.
Plantar (Babinski)
Warn the patient
Using an orange stick, gently scrape the plantar surface of their foot in a semi-circle from the heel, around the lateral edge and to the ball of the big toe
Big toe ↑ = UMN lesion; big toe ↓ = normal
Co-ordination
Heel-to-shin test
Ask the patient to touch their heel to their contralateral knee
Then ask them to slide their heel down the tibia to their contralateral ankle
Now ask them to move it back up, through the air, to their contralateral knee again
For pain and light touch, first show the patient how each should feel on their sternum, then start distally. If there is distal sensory lossor if from the motor exam you suspect ‘glove and stocking’ sensory loss, or a sensory-level, test from distal to proximal in 2-3 straight lines. If distal sensation is intact, or if from the motor exam you suspect nerve/nerve root pathology, test dermatomes ± peripheral nerves:
Pain (spinothalamic)
Use neurological pin
‘Close your eyes and say “yes” every time you feel the pin. Please also let me know if it feels blunt.’
Light touch (dorsal column)
Touch the skin with a cotton wool ball (don’t stroke it)
‘Close your eyes and say “yes” every time you feel the cotton wool.’
For the modalities below, start distally and only move proximally if the patient cannot feel you:
Proprioception (dorsal column)
Hold the proximal phalanx of the patient’s big toe with your index finger above and your thumb below
Move the distal phalanx up and down with the thumb and index finger of your other hand, holding it on each side
Show the patient the up and down positions
Now ask them to close their eyes and repeatedly wiggle the distal phalanx up and down. Stop in one position and ask them if it is up or down. Do this three times.
If they get it wrong, move to the metatarsophalangeal joint, then the ankle, and so on until they can correctly state the position
Vibration (dorsal column)
Twang the prongs of a 128Hz (long) tuning fork
Place the round base on their sternum to demonstrate how it should feel
Now ask them to close their eyes and hold it over the interphalangeal joint of their big toe. Ask if they can feel it vibrate and when it stops vibrating. (Grip the prongs to stop the vibration yourself.)
If they cannot sense the vibration, move to the metatarsophalangeal joint, then medial malleolus, then tibial tuberosity, and so on until they can
Temperature (spinothalamic)
Use the prongs of the tuning fork on the patient’s sternum to test if they can identify them as cold
If so, touch a prong horizontally to the skin on the dorsum of the distal foot and ask if the patient can feel it as cold. If not, move proximally up the leg until they can
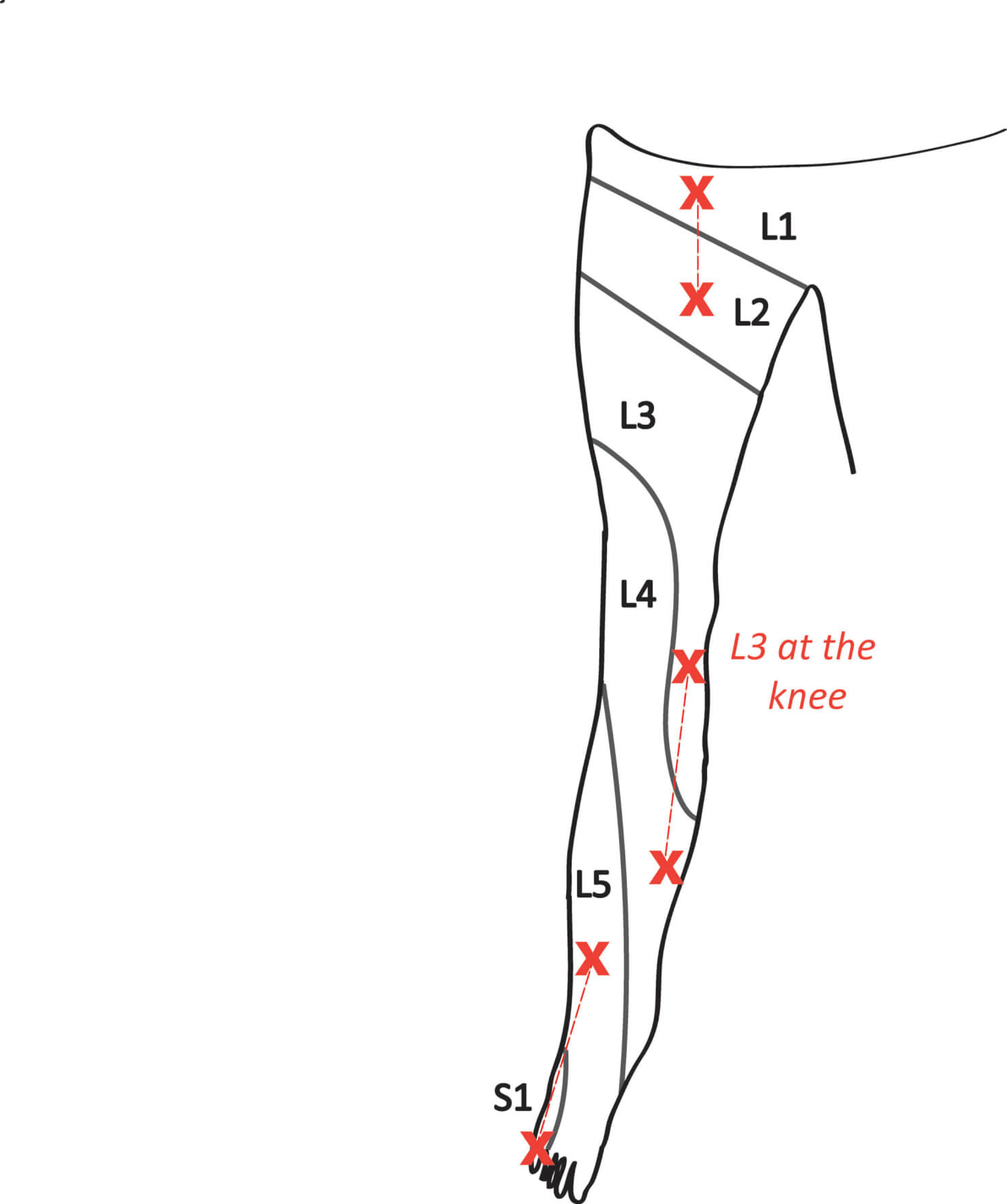
Lower limb dermatomes
To complete
Thank patient and restore clothing
‘To complete my examination, I would examine the cranial nerves and perform an upper limb neurological examination.’
Summarise and suggest further investigations you would consider after a full history
Clinical features of upper and lower motor neuron lesions