A systemic type I (IgE mediated) life-threatening hypersensitivity reaction. 10-20% of cases may not have skin/mucosal changes (i.e. just bronchospasm or hypotension).
Initial actions
Immediately get help, call medical emergency team on 2222 (tell switchboard it is a medical emergency and the location) and remove allergen (i.e. stop any infusions).
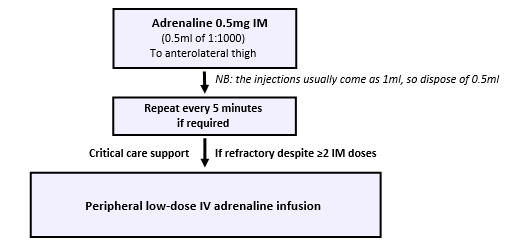
Adrenaline administration
Airway
Secure airway
If stridor/airway obstruction, adrenaline nebuliser (5ml 1:1000) and consider intubation
Breathing
Apply sats probe
Attach 15L/minute oxygen via a non-rebreather mask
Bag-mask ventilation or intubation if apnoeic
If wheeze, salbutamol (5mg) and ipratropium (500mcg) nebulisers with oxygen
ABG
Circulation
Check blood pressure and apply 3-lead cardiac monitoring
Secure IV access (2 large-bore IV cannulas) – get IO access if unable to estabish IV access
IV fluids 500-1000ml 0.9% saline/Hartmann’s solution STAT fluid challenge initially (may need 3-5L IV fluids – give as fast as needed and titrate to BP)
Take bloods (including mast cell tryptase) and blood gas