2. Taylor francis 🧠: over 2500+ questions licenced from 18 text-books worth £191
3. Past examiners 🫁: Questions written by previous Medical School examiners
4. Track your performance 🏃♀️: QBank uses intelegent software to keep you on track
The reviews are in
★★★★★
6,893 users
Don't take our word for it
"The stations you provide are strikingly similar to those I came across during my medical school finals (some even verbatim!), and I have tried many other exam platforms. I'm truly grateful for your priceless support throughout my final couple of years at medical school!"
Raza Q 🇬🇧
"It has absolutely everything for medical school, so many histories with detailed differential diagnoses, how to approach emergencies, commonly prescribed drugs..every kind go examination you’ll ever need in osces"
John R 🇬🇧
"Thank you SO MUCH for the amazing educational resource. I’ve tried lots of platforms and books with mock OSCE stations and yours is by far and away the best I’ve tried"
Ed M 🇳🇿
"Get this right away. So helpful for OSCEs but also general clinical learning and understanding. Wish I had brought it sooner"
Emma W 🇬🇧
"Without a doubt, your platform outshines all other OSCE resources currently available. In all honesty, I can confidently attribute my success in securing a distinction in my finals to OSCEstop."
Harish K 🇬🇧
"OSCEstop distinguishes itself from many other platform banks by offering a wealth of questions that mimic the demanding and complex aspects of our finals. This platform played a crucial role in ensuring I was ready for the level of difficulty that awaited me in my final exams."
Membership includes access to all 4 parts of the site:
1. Learning 📖: All notes, viva questions, track progress
2. Stations 🏥: 10 years of past medical school stations. Includes: heart murmurs, ECGs, ABGs, CXR
3. Qbank 🧠: 2500+ questions from Taylor Francis books, complete MLA coverage
4. Conditions 🫀: all conditions mapped to MLA, progress tracking
The reviews are in
★★★★★
6,893 users
Don't take our word for it
"The stations you provide are strikingly similar to those I came across during my medical school finals (some even verbatim!), and I have tried many other exam platforms. I'm truly grateful for your priceless support throughout my final couple of years at medical school!"
Raza Q 🇬🇧
"It has absolutely everything for medical school, so many histories with detailed differential diagnoses, how to approach emergencies, commonly prescribed drugs..every kind go examination you’ll ever need in osces"
John R 🇬🇧
"Thank you SO MUCH for the amazing educational resource. I’ve tried lots of platforms and books with mock OSCE stations and yours is by far and away the best I’ve tried"
Ed M 🇳🇿
"Get this right away. So helpful for OSCEs but also general clinical learning and understanding. Wish I had brought it sooner"
Emma W 🇬🇧
"Without a doubt, your platform outshines all other OSCE resources currently available. In all honesty, I can confidently attribute my success in securing a distinction in my finals to OSCEstop."
Harish K 🇬🇧
"OSCEstop distinguishes itself from many other platform banks by offering a wealth of questions that mimic the demanding and complex aspects of our finals. This platform played a crucial role in ensuring I was ready for the level of difficulty that awaited me in my final exams."
Please note OSCEstop content is for educational purposes only and not intended to inform clinical practice. OSCEstop and authors take no responsibility for errors or the use of any information displayed.
Roles of the team leader
Delegate tasks (leader should be hands-off)
Timer and scribe (keep this person close to you and ask them to clearly tell you when each cycle ends, the cycle number and remind you when drugs are due if competent to)
Compressions (2-3 people rotating)
Airway and ventilation (anaesthetist if present)
Defibrillation (if shockable)
IV access, bloods/gases and drugs (x 2 people)
Co-ordinate above tasks
Go through reversible causes
DR’s ABCD
Danger: check around patient and environment for danger
Response: question (e.g. ‘Hello, can you hear me?’), shake and command (e.g. ‘Open your eyes’)
Shout: ‘Can I get some help over here please?’ and make the bed flat
Airway: open airway with head-tilt/chin-lift or jaw-thrust and look for obstructions
Breathing: assess breathing for up to 10 seconds by listening and feeling with your ear, while watching for chest movements and palpating carotid pulse
NB: you should do this while maintaining the head-tilt/chin-lift or jaw-thrust (e.g. place your forearm on the patient’s forehead, apply positive pressure to tilt the head back, and reach around their face to pull up the angle of the jaw with the index and middle fingers, whilst palpating the carotid pulse with the other hand).
CPR and Call cardiac arrest team: if patient is not breathing, start CPR (described in detail below) and ask a helper to call 2222 and explain there is an adult/paediatric/neonatal/trauma cardiac arrest and the location. Ask the helper to bring the resuscitation trolley back with them.
Defibrillation: as described below
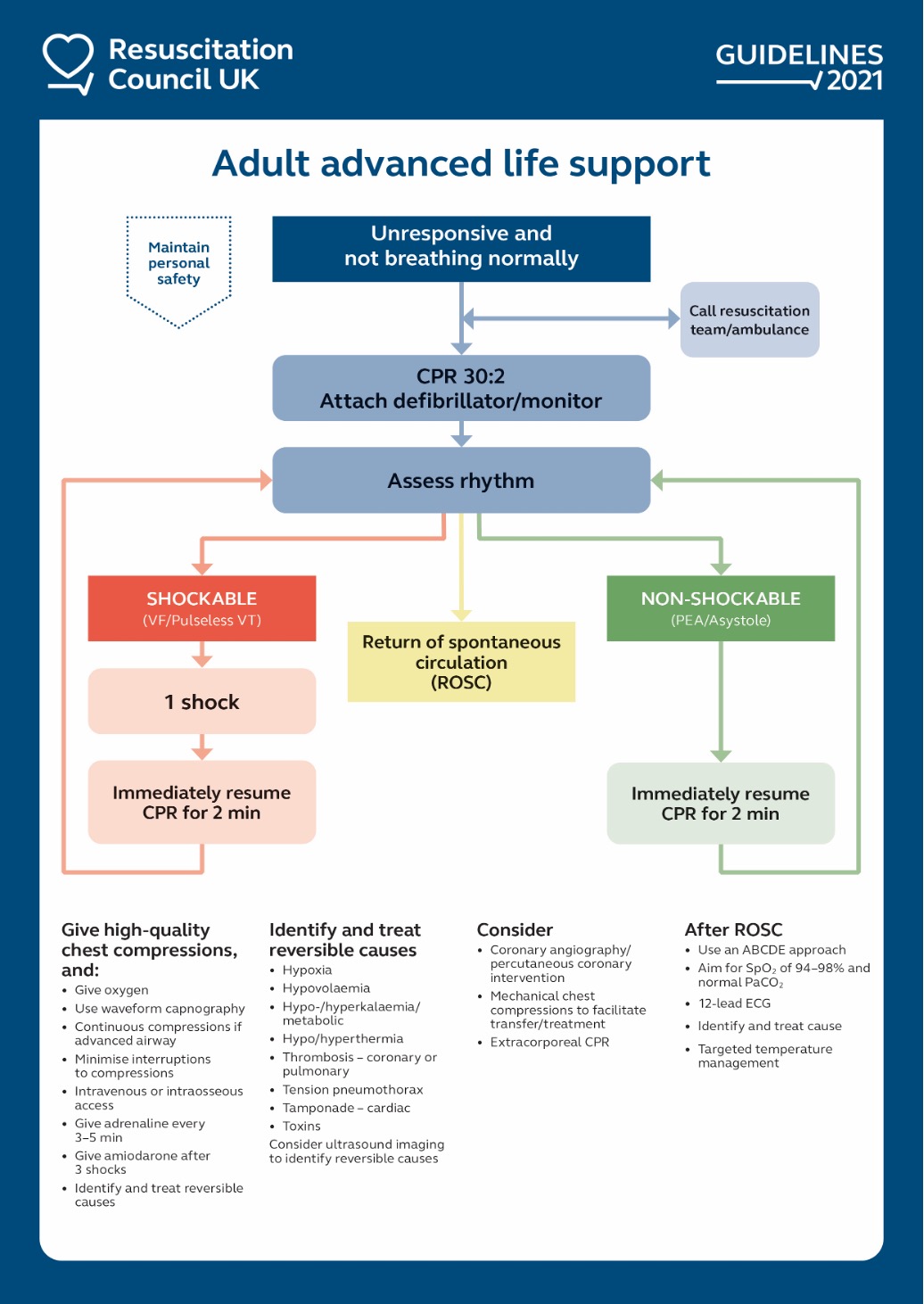
Tasks needing to be performed simultaneously are shown below in order of priority:
Chest compressions
Perform 30:2 chest compressions to ventilations (until airway is secure).
Perform at a rate of 100-120/minute (i.e. 2/second) and a depth of 5-6cm. Fully extend your elbows, wrists and fingers. Have both hands palm downwards with fingers interlocked. Place the carpal area of the hand over the lower sternum and apply all pressure over this point.
ONLY stop CPR for rhythm checks, electrical shocks, and the 2 rescue breaths. Ask the person doing compressions to tell the airway person each time 30 compressions are complete.
Chest compressions should be continuous once the airway is secured with endotracheal tube
Switch CPR provider during the rhythm check every 2 minutes (or earlier if they tire)
Compression technique
Defibrillation
Setup
Working around the person performing compressions, place the two defibrillation pads in the correct positions on the chest (below right clavicle and over cardiac apex). You may need to shave or dry the chest. Leave jewellery on, but move it out the way.
NB: if an implantable device is present, ensure pads are >8cm away from it (you can put the pads on AP if needed)
Connect pads to defibrillator (and set monitoring trace to ‘pads’ if not already)
Delegate someone to manage timing, clearly tell the leader when 2 minute cycles are up and remember the cycle number. Cycle 1 starts when the defibrillator is connected.
Defibrillator pad position
Rhythm check
Perform a rhythm check ± shock every 2 minutes
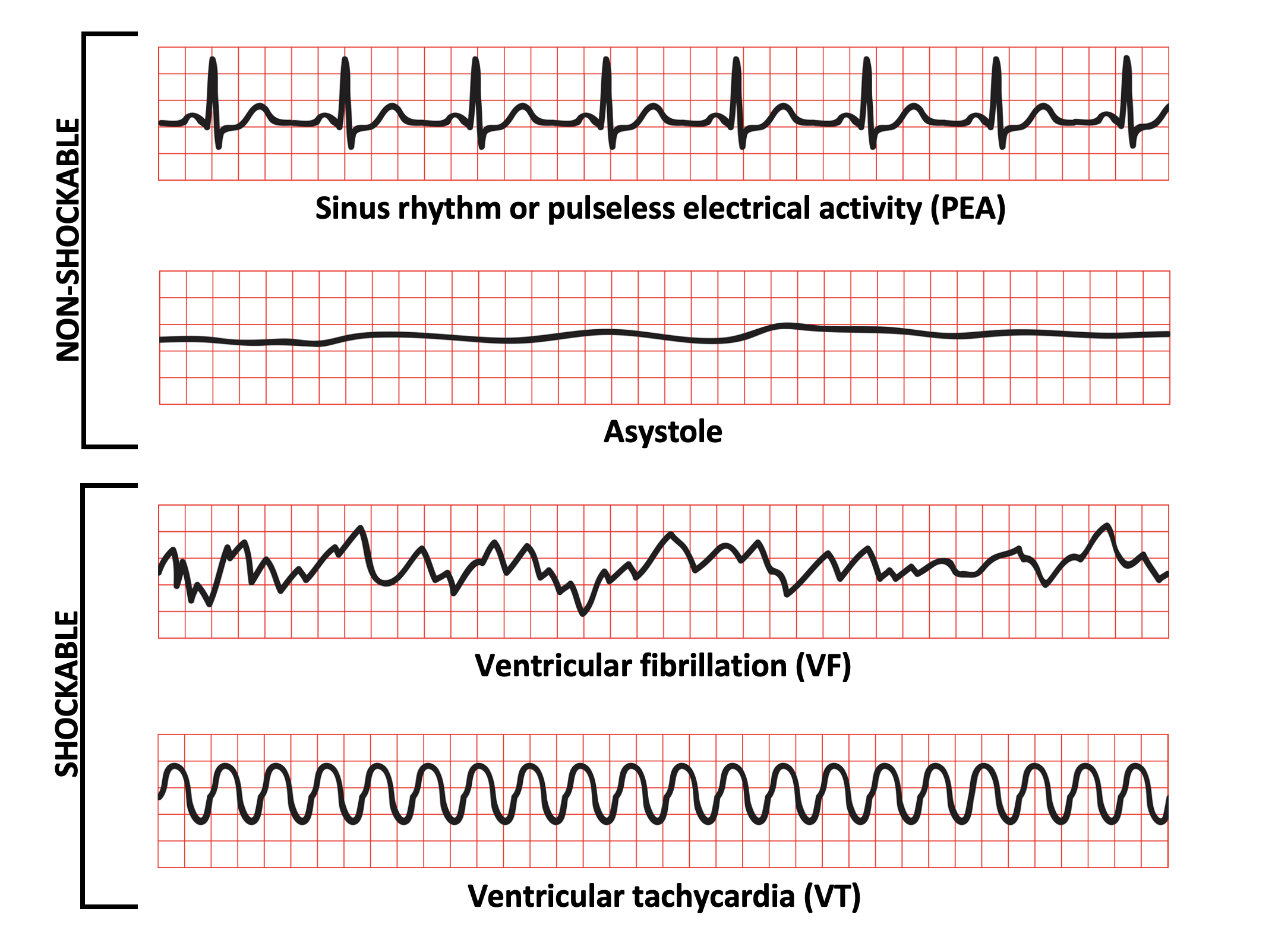
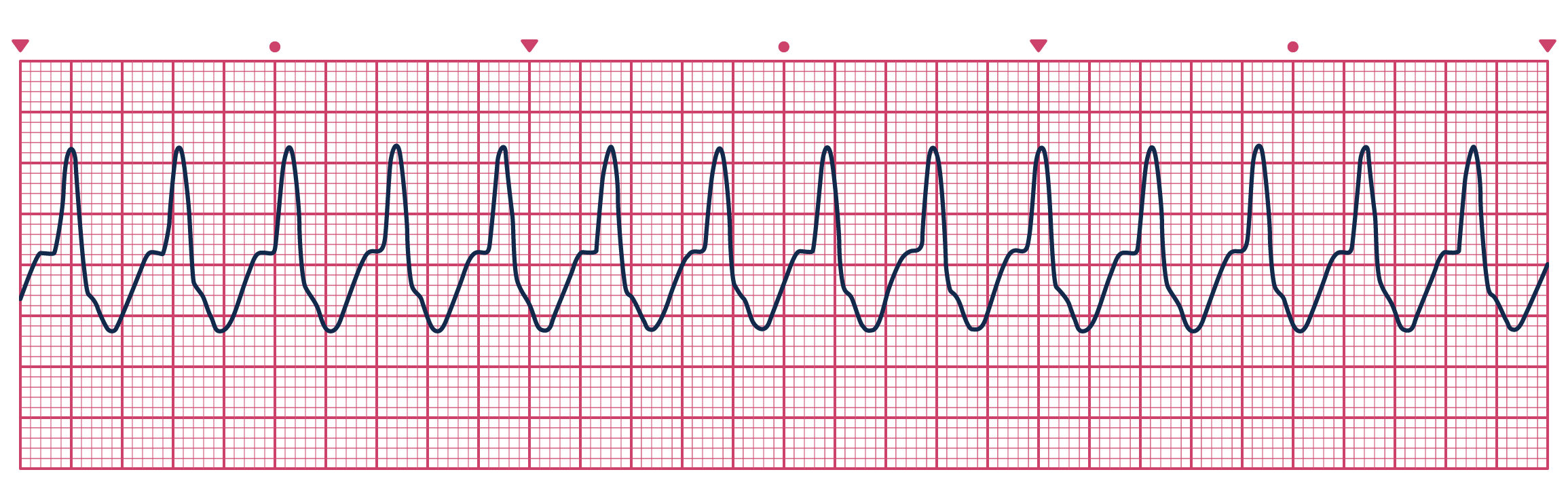
When pads are in place and defibrillator is on, immediately ask for CPR to be stopped for a rhythm check. Determine if the rhythm is shockable (‘wavy lines’ – VF, VT) or non-shockable (asystole, PEA).
If a rhythm that could be compatible with a pulse is seen (i.e. sinus or VT) during the rhythm check, also feel for a central pulse and stop compressions if present
Then immediately continue CPR
Shock
If shockable rhythm, follow these extra steps:
Select correct energy level for device (e.g. 150J biphasic).
Ask for oxygen to be removed (unless patient intubated) and everybody except the person doing compressions to move away. Tell the person doing compressions to continue and that you will alert them to move away before the shock.
Charge defibrillator by pressing ‘charge’ and then move hand away from machine
Once charged, ask the compressions to now be stopped and that person to move away and shout ‘Everybody stand clear!’
Check the area is clear (i.e. check no one is in contact with the patient/bed and that the oxygen is away)
Deliver shock by pressing ‘shock’
Immediately ask for CPR to be restarted
NB: while operating defibrillator, always look outwards around the bed (not at the machine) and never float your hand near the buttons.
Bag valve mask (30 compressions to 2 ventilations): if able to ventilate whilst maintaining seal and jaw-thrust, one person can do this alone. If not, one person should hold the rigid part of the mask with their thumb and index finger (‘C’) and pull the jaw up into the mask with their other fingers (‘E’), while another person ventilates.
Consider also placing an oropharyngeal (Guedel) or nasopharyngeal airway under the mask if struggling.
Supraglottic airway (usually i-gel): more secure airway and easy to insert
Intubation with endotracheal tube (gold standard): only done by experienced personnel. Once placed, ventilate every 6 seconds with continuous chest compressions and oxygen does not need to be removed for shocks.
NB: if a supraglottic airway is placed and there is no air leak, compressions can also be continuous and oxygen left connected for shocks. In practice, however, there is usually still some air leak so this is usually not done.
Attach 15L/minute oxygen
Attach waveform capnography if supraglottic mask or endotracheal tube inserted
Avoid hyperventilation
Drugs
Obtain IV access and have drugs ready
If you cannot get IV access after 2 attempts, get intraosseous access via head of humerus or tibial tuberosity
Take blood from the cannula (VBG + send FBC, U&Es, Mg2+, G&S) and give IV fluids
Adrenaline 1mg IV (10ml of 1:10,000)
When to give
Shockable rhythm: give after 3rd shock (during CPR). Flush with 20ml saline.
Non-shockable rhythm: give as soon as IV access is established. Flush with 20ml saline.
Repeat adrenaline dose during every other CPR cycle thereafter (i.e. repeat every 3-5 minutes once given, regardless of rhythm)
Amiodarone 300mg IV: if shockable rhythm only. Give after 3rd shock (during CPR). Repeat 150mg IV after 5th shock if ongoing.
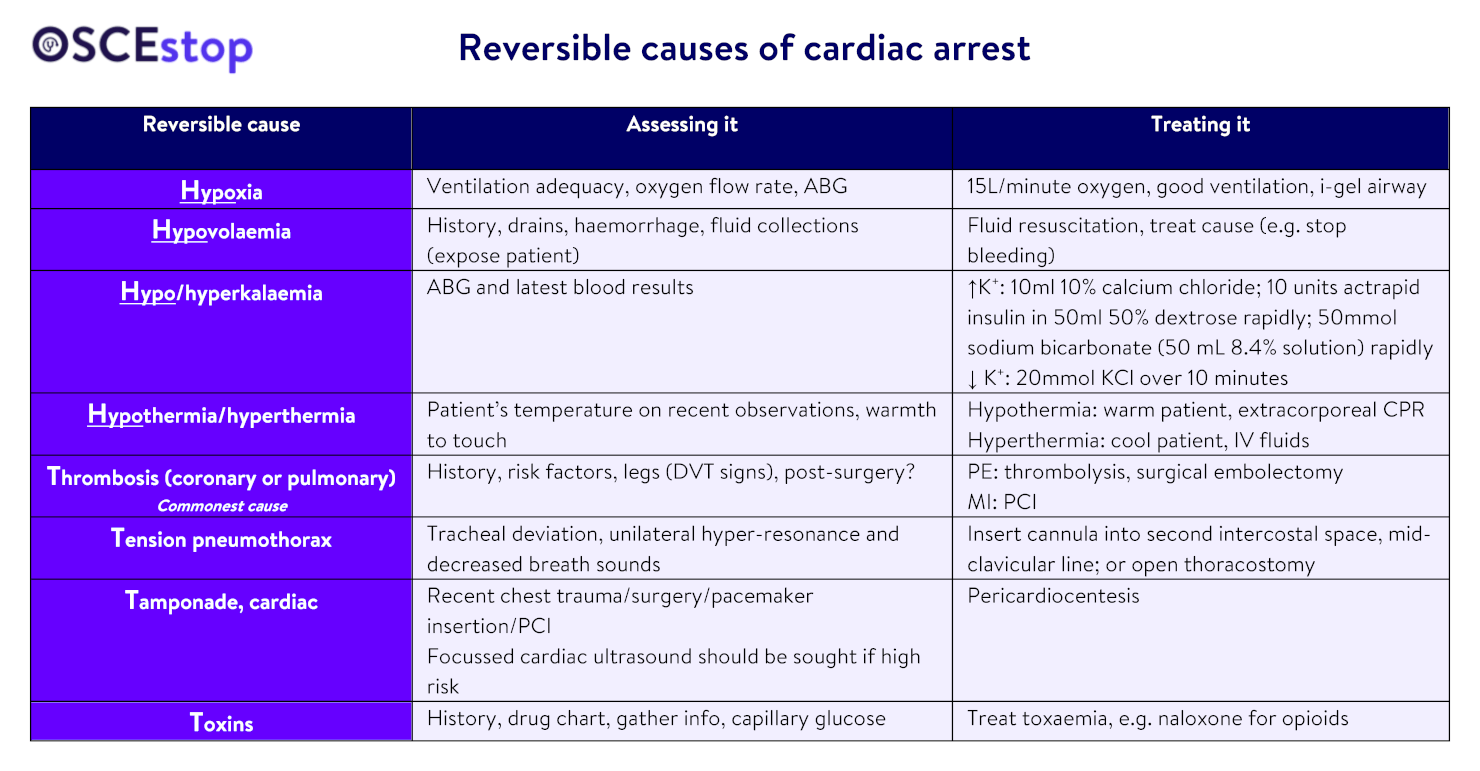
Consider reversible causes
The team leader should assess the reversible causes by assessing the patient, speaking to nurses/relatives and reviewing their drug chart and notes. Each of the following reversible causes should be eliminated/treated (4 H’s, 4 T’s):
What next?
Return of circulation
Full ABCDE assessment
Controlled oxygenation (aim 92-96%)
Consider therapeutic hypothermia 32-36˚ for 24 hours (avoid hyperthermia)
Post-arrest investigations
Treat cause
Consider transfer to intensive care if still requiring ventilation or high-dependency care if not
No return of circulation
In general, CPR should be continued as long as there is a shockable rhythm (mechanical compression device may be used)
Only stop if a registrar or above makes the decision with the team
Extracorporeal CPR using extracorporeal membrane oxygenation (ECMO) device may be considered where available for select patients to facilitate other definitive treatments, e.g. PCI, pulmonary thrombectomy for massive PE, rewarming for hypothermia
Afterwards → Retrospectively document everything that happened




thanks
I appreciate all your hard work
Great to hear, thanks! 😃
Thank you for the helps
Great to hear, thanks! 😃
[…] https://oscestop.education/acutely-unwell-patients/adult-advanced-life-support/ […]