Please note this information is for educational purposes only and procedures should not conducted based on this information. OSCEstop and authors take no responsibility for errors or for the use of any content.
Indications: haemodynamically unstable bradycardia (unresponsive to atropine); complete heart block; Mobitz type II second-degree heart block when haemodynamically unstable; sudden witnessed asystole secondary to cardioversion/drugs/conduction defect; override pacing of tachycardias refractory to drugs and cardioversion (rarely used)
Setting up
Anaesthetist must be present to sedate patient (most patients cannot tolerate pacing >50mA)
Apply 3-lead cardiac monitoring (clockwise from right arm Ride Your Green Bicycle) and connect lead to external cardiac monitor or defibrillator machine
Red: anterior aspect of right shoulder
Yellow: anterior aspect of right shoulder
Green: left anterior superior iliac spine
Black: not present on defibrillation machine
Apply defibrillator pads (in AP position) after shaving chest if required
‘Right’ pad: place longitudinally on left sternal edge
‘Left’ pad: place longitudinally on left paraspinal muscles (in line with anterior pad)
Connect pads lead to defibrillator machine
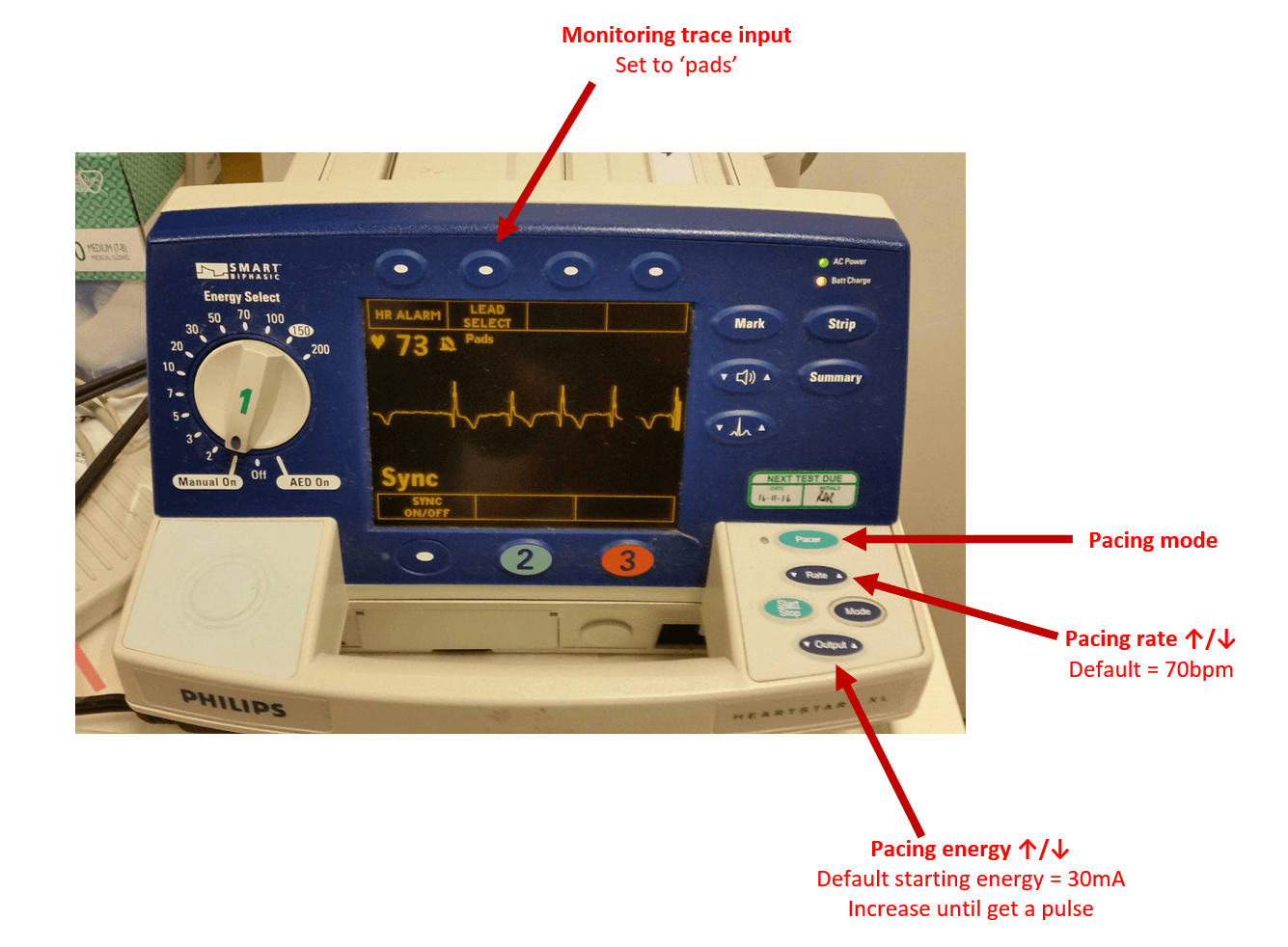
Set defibrillator machine monitoring trace to ‘pads’
Pacing
Set defibrillator to pacing mode
Set onscreen pacing rate (default usually ̴ 70bpm) and energy (default starting energy usually ̴ 30mA)
Click onscreen start pacing button
Observe the monitor to see if QRS complexes follow every pacing spike – if not, increase the energy until they do – ‘electrical capture’ (usually occurs at 50-100mA)
Next check the patients pulse corresponds to the induced QRS complexes – ‘mechanical capture’

Comments are closed for this post.