<6months = high-risk because present with non-specific symptoms (lethargy/irritability, poor feeding, reduced urine output) and may look well even when very unwell
Most viral
Be wary of serious causes (!), if the child is very young and if there is no obvious source
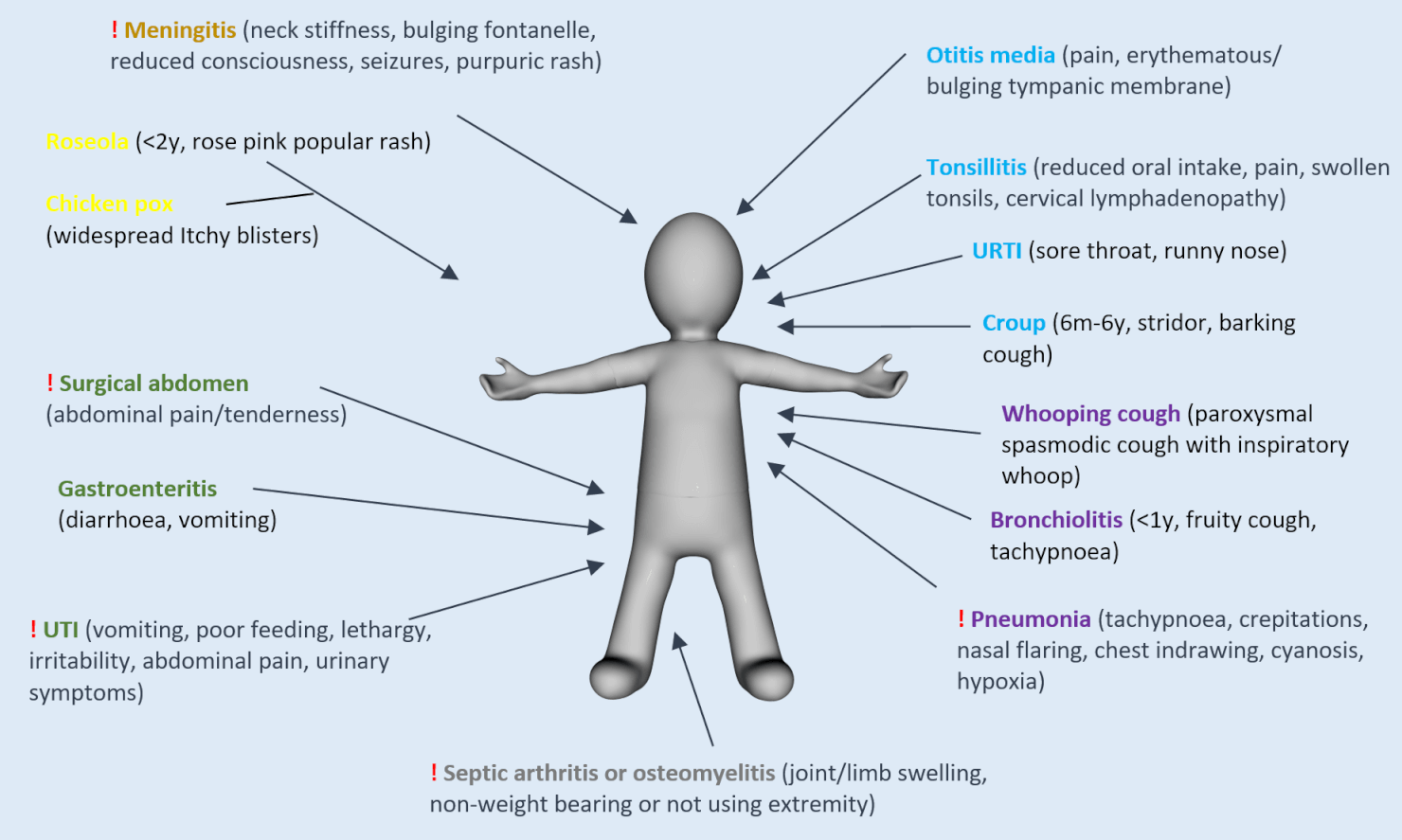
Common causes of fever in a child
Many other causes e.g. infectious mononucleosis, slapped cheek syndrome, pharyngoconjunctival fever, hand foot and mouth, measles, mumps, rubella, epiglottitis, scarlet fever, Kawasaki disease, encephalitis, rheumatic fever, endocarditis, malaria, TB, post-vaccination fever etc
Only do investigations that will change management
At risk groups
<3months = full septic screen regardless (including LP)
<6months or unwell = full septic screen if no source found
Possible investigations – BOXES
Bloods: FBC, CRP, U&E, cultures, VBG, glucose (hypoglycaemia common in unwell babies/infants)
Orifice tests: urine dip and culture (next thing to do if no source found in exam; parents to wait with sterile pot; in and out catheter may be used in young children if waiting too long); stool culture (if diarrhoea)
X-rays/imaging: CXR (if respiratory signs)
ECG (if HR>200 – ?SVT)
Special tests: lumbar puncture (if <3months or very unwell or meningitis suspected)
A 14 year old with tonsillitis was given amoxicillin and represents with ongoing fever and a maculopapular rash. What is the likely cause of illness? Which laboratory abnormalities may be seen on basic blood tests?
A 1 year child with a history of tetralogy of Fallot repair presents with a fever and is found to have splinter haemorrhages. What are the diagnostic criteria for infective endocarditis?

Comments are closed for this post.